

Antigenic Original Sin; Was Mass Vaccination Against Covid The Right Move?

I. Immune Imprinting
Introduction
When our immune system first encounters a new bug, such as a virus, it creates from it a kind of blueprint or ‘mold’ for self-defense that it can call upon for quick action during subsequent exposures to the same microorganism–a process known as immune imprinting.
That both infections and vaccinations can induce immune imprinting is not a new finding in the field of immunology. In fact, it was Jonas Salk who first observed it (his team referred to it as 'antigenic original sin'). But the importance of immune imprinting–including its role in decreasing the effectiveness of the current Covid vaccines–has been getting a lot more attention recently.
The Immune System Punches with Two Arms
Each compartment of our immune system has two distinct arms: adaptive and innate. Imprinting occurs within the adaptive arm which is made up mainly of B cells, T cells, and antibodies. Adaptive immunity expands and learns over time as each new exposure to a novel microorganism causes the cells that pump out antibodies, called B cells, to imprint new molds which they reserve in immune hubs like lymph nodes and bone marrow for the rest of our lives. If we are ever exposed to the same bug again, those reserved B cells, called memory B cells, are induced to quickly mature into plasma cells and start pumping out antibodies using their imprinted ‘antibody molds.’
The problem is that, if an immune imprinted microorganism becomes endemic (permanent, stable, and predictable), as SARS-CoV-2 has now become, and mutates substantially over time to give rise to clinically significant new strains, as it has done will likely continue to do, then subsequent exposures to new strains will induce an immune response that is tailored more toward the original strain of the bug than the current ones. And over time, the problem gets worse as each new variant becomes sequentially more different from the original and a progressively larger share of the antibody production by imprinted B cells becomes ineffective.
We’ve All Been Imprinted Against SARS-CoV-2
By now, almost everyone has either been infected, vaccinated, or both against one of the early strains of SARS-CoV-2. And, as a result, we now harbor reserved memory B cells imprinted by that early strain. When the Covid vaccines were first rolled out in January 2021, the Alpha variant, which had mutated only a short distance from the genome of the original Wuhan-Hu-1 strain, had just reached our shores. At that time, the antibodies made from the imprinted molds of the memory B cells among vaccinated persons, though not perfectly matched to Alpha, were still close enough to be extremely effective. And if the virus made its way into our cells to cause an infection, we had a well-trained army of T cells to pounce on it and shut the infection down.
In fact, two weeks after I received my second shot, I resumed seeing vaccinated patients unmasked in exam rooms that had minimal ventilation. And it was safe to do so because my immunity was > 90% effective at preventing me from catching or spreading Covid.
Today, however, while being vaccinated offers our immune systems the head-start they need to prevent, in most cases, severe illness or death, many of the antibodies we are pumping out are no longer effective because they are matched to dozens of epitopes (areas) on the original spike protein of the Wuhan-Hu-1 strain that no longer exist on the current variants of the virus.
More importantly, our imprinted molds don’t seem to be doing a good job of making the updated antibodies that we need to gum up the new epitopes on the new variants when we are exposed to them. A recent study published in Nature demonstrated that people who had been vaccinated against the original strain and then got infected by Omicron produced antibodies against epitopes that were common to both Wuhan-Hu-1 and Omicron but not against those found only on Omicron. By contrast, those without a previous vaccination or infection exclusively made antibodies that matched Omicron. That study would be difficult to replicate today, now that China has 'reopened,' as it would be extremely rare to find adult subjects who have never been either infected or vaccinated.
In the Rearview Mirror
So, was mass vaccination a bad idea? At least one veterinary virologist/vaccinologist, Geert Vanden Bossche, has advanced the hypothesis that widespread vaccination against SARS-CoV-2 may be accelerating the virus’ evolution by putting selective pressure on it to change its spike protein in order to evade our imprint-derived antibodies, leading to the emergence of progressively more infectious variants. Vanden Bossche refers to this as “vaccinating into a pandemic,” something he believes will turn out to have been a bad idea in the long term.
It is even possible, Vanden Bossche points out, that weakly binding or non-neutralizing antibodies caused by vaccine-induced immune imprinting can be causing the virus to become more infectious through a mechanism known as antibody-dependent enhancement (ADE). The spike protein of SARS-CoV-2 can change its shape to be either open or closed. In order for the virus to infect our cells, the spike must be in the open position where it is able to bind to our cells’ membranes. Certain weakly binding antibodies made from imprinted molds may cause the spike protein to stay permanently open, enhancing its ability to cause infection.
Unfortunately, there has been so much anti-vaccine pseudo-science and disinformation in ‘conservative media’ that voices like his, raising interesting questions that challenge the consensus understanding informing Covid strategy, have been dismissed as nonsense rather than debated thoughtfully among the responsible media, where a kind of hypervigilance against harmful disinformation has understandably developed.
That said, it is important to bear in mind that both vaccines and infections cause immune imprinting so both can also potentially put selective pressure on the virus to mutate and both can potentially cause ADE. Early versions of the RSV and measles vaccines, for example, did induce some degree of ADE (and were, therefore, appropriately discontinued). Infection with dengue can cause ADE and so can the dengue vaccine, so its use has been limited to only those who are not at risk for developing ADE (dengue has four distinct viral clades and the vaccine must match the clade to avoid ADE). Critically, with respect to Covid, no evidence of ADE has emerged in response to either vaccinations or infections.
Anti-vaxxers should know that unvaccinated people infected by the Alpha variant made Alpha-specific antibodies when they were subsequently reinfected with Omicron. And should those same unvaccinated people who had been infected first by Alpha and then by Omicron, get infected yet again, this time with XBB.1.5 (which currently accounts for three-fourths of all cases in the US), they will likely still pump out mainly or perhaps even exclusively Alpha-specific antibodies, some of which will be weakly binding or ineffective. In short, whether you have immunity today because of vaccination or infection, you’re immune imprinted but no evidence has yet emerged (and it should have by now if this were an issue) for ADE, either after vaccinations, infections, or both.
In the end, vaccination was estimated to have saved twenty million lives, globally, just during 2021. It may turn out that there is a downside to having engaged in mass vaccination but there are no compelling data to suggest that so far. I’ve had five shots and will likely now wait until a new, better vaccine (see below) becomes available before taking my next booster.
Why is this So Meaningful Now?
Thanks to mRNA and other new technologies, it’s now relatively easy to update vaccines to match new strains. But imprinting implies that strain-specific vaccine boosters in and of themselves should not offer dramatically better protection against infection, transmission, or progression of illness severity compared to boosting with the original vaccine. And that is what the data are showing regarding the current bivalent vaccine which has been updated to the BA.5 Omicron lineage.
This new vaccine, given as a third, fourth, or fifth shot, despite being tailored to BA.5, induces the production of antibodies that are mainly tailored to the original Wuhan-Hu-1 strain, offering only about 37% better protection (with 62% overall protection) against developing severe disease if infected by BA.5 or one of three other contemporary Omicron lineage variants, compared to a booster shot of the original vaccine. However, the value of this modest boost in effectiveness is questionable as the data from the two groups used to make the comparison were collected at different times and did not control for the prescription of Paxlovid which was far more available during the latter period of time when the group who received the updated bivalent booster was studied. In short, if the current bivalent booster offers extra protection compared to the original vaccine, the degree of that extra protection is probably quite modest.
This is a general story about large populations of people with some expected individual variation. Some vaccinated and/or previously infected people make no amount of new antibodies on exposure to new strains (strong immune imprinting) while others make varying amounts of new antibodies. This study looked at the immune responses of people who had contracted an Omicron infection after having been triple vaccinated (with the original vaccine built against Wuhan-HU-1) but with various infection histories. They saw a variety of subtly differing immune responses indicating varying degrees of imprinting linked to varying histories of previous exposures.
For example, among triple vaccinated people whose first Covid infection was with Omicron, their antibodies were best matched to the original Wuhan-Hu-1 strain and progressively less well matched to each subsequent variant (Alpha, Delta, Omicron). Their immune response showed some effects of imprinting but they were able to produce a small amount of Omicron-specific antibodies, probably by generating new B cells with updated molds. However, among those who had first been infected with the original Wuhan-Hu-1 strain and then subsequently (triple) vaccinated against it, a subsequent Omicron infection didn’t generate any Omicron-specific antibodies at all.
Immune Evolution (Affinity Maturation)
One of the many wondrous things about our immune systems is that those memory B cells living in immune hubs after an infection, waiting to be called upon to mature into plasma cells that pump out antibodies from their imprinted molds, undergo genetic mutations of their own. Over time, they subtly and gradually alter their molds to make new antibodies that do not match the original strain but might match future strains of that same bug. Memory B cells, in other words, engage in a kind of conscious evolution engineered to predict how infectious microbes will themselves change over time–something called affinity maturation–and we are seeing this happening with regard to SARS-CoV-2.
Unfortunately, affinity maturation is not going to get us out of the Covid problem. B-coronaviruses are generally much more stable than SARS-CoV-2 has turned out to be and, with regard to Covid, viral evolution is clearly outpacing memory B cell evolution. But thankfully, we have other tricks up our sleeves.
II. Vaccine Evolution
Influenza as an Example
The current pandemic caused by SARS-CoV-2 hardly represents the first time that we have ‘vaccinated into a pandemic.’ In a functional sense, we have been doing this every year for decades to protect ourselves against the flu. Influenza, like SARS-CoV-2, is a virus that evolves very quickly, resulting in multiple clinically significant new variants each year. We address this problem, in part, by updating the vaccines annually to immunize us against the strains that experts predict will become predominant by the time winter rolls around and people start spending more time indoors, in group settings, where their germs are easily spread around. But why would annually-updated variant-specific vaccines work against influenza but not against SARS-CoV-2?
Adjuvants
Despite immune imprinting, flu vaccination has been an effective defense strategy for a couple of reasons. First, influenza is not nearly as deadly a virus as SARS-CoV-2, nor does it routinely cause ‘long-flu’ or ‘post-flu conditions', so a moderate degree of protection afforded by updated, variant-specific vaccines each year offers a good enough barrier of protection for most healthy adults (flu vaccines are typically about 50% - 65% effective). And secondly, we include adjuvants in flu vaccines that supercharge their effectiveness.
Adjuvants are substances that enhance the immune response to a vaccine by stimulating not the adaptive arm of the immune system (those B cells, T cells, and antibodies) but the innate immune response. Increased production of the cells of innate immunity (macrophages, dendritic cells, and lymphocytes) which are always patrolling the body looking for foreign agents, is stimulated by adjuvants like aluminum salts, oils, and virosomes. By augmenting the innate response, adjuvants can help compensate, to some degree, for the limitations of adaptive immunity caused by immune imprinting. And there is now talk of adding adjuvants to the Covid vaccines as we have done for years with flu vaccines.
A New Method of Delivery for the Covid Vaccines
The immune system is far more complex than the limited story that I learned in school 35 years ago about innate and adaptive immunity. We now know, for example, that there are also different compartments of the immune system that oversee distinct territories of the body and are capable of acting independently from one another.
One such immune compartment called the MALT (mucosal-associated lymphoid tissues), is responsible for protecting the mucosal linings of the airways and gut. These are the areas that first make contact with many of the most common germs that can make us sick. Cold and flu viruses, RSV, various bacteria that can cause food poisoning, norovirus (currently on the rise), and SARS-CoV-2 all enter our bodies through the mouth and/or nose where they attempt to latch onto the cells that line the throat, lungs, nasal passages, and gut (mucosal epithelial cells).
When a bug enters the nose or mouth, the innate arm of the MALT kicks in first. Coughing, sneezing, runny/stuffy nose, and diarrhea are all symptoms of innate immunity in the MALT–attempts to expel or wash out the bug before it has a chance to gain a foothold on epithelial cells to cause infection. That mucous also contains innate immune cells, such as macrophages that can gobble up infected cells and destroy the viruses inside them. Meanwhile, memory B cells are called up and within a few days of the initial exposure, the adaptive arm of the MALT begins pumping out its own special class of antibodies called IgA.
IgA is particularly good at gumming up viruses trapped in mucous, thereby preventing them from latching onto our cells. IgA makes its way into the lungs, throat, nose, and gut via mucous secreted by those same mucosal epithelial cells. By day four or five after an exposure (sooner if the MALT has been primed by prior infection or vaccination), a runny, stuffy nose represents more than just an attempt to expel the virus (innate immunity), it is also an attempt to flood the zone with IgA (adaptive immunity).
When we shoot a vaccine into an arm muscle, as we have done with the Covid vaccines so far, we bypass the MALT, engaging instead what is often referred to as the Generalized Immune System. Because the current intramuscular Covid vaccines fail to prime the MALT, they do not induce the production of robust levels of IgA. This is another reason why the current vaccines are not doing a great job of protecting us against getting infected or spreading the virus. And it is the reason that I've been writing for some time about the need to switch from intramuscular to mucosal vaccination that engages the MALT.
Mucosal vaccination (vaccines delivered in the form of nasal drops or inhaled via nebulizer) directly engages the MALT, inducing the production of B cells, T cells, and robust levels of IgA.
Once immunized, the MALT can flood the mucosal tissues of the nose, throat, lungs, and gut with IgA immediately upon inhaling or swallowing the virus. Gumming up the virus while it is still in the mucous of our airways before it has had a chance to invade our cells, offers the best protection against infection. And if the virus does make its way through the mucous without getting gummed up by IgA, the MALT has T cells that can be trained via mucosal vaccination to attack and destroy the infected epithelial cells, preventing the virus from making its way into the interior of the body.
Priming the MALT through mucosal vaccination likely offers the best hope for halting the spread of the disease, preventing long-Covid and post-Covid conditions (such as heart attacks and strokes), and making it safe to return to things like indoor socializing without the risk of catching or spreading Covid.
But.. Why Bother When Covid Isn’t Killing People Anymore?
The deadliness of Covid has been widely reported to dwarf that of more common infectious diseases like the flu.
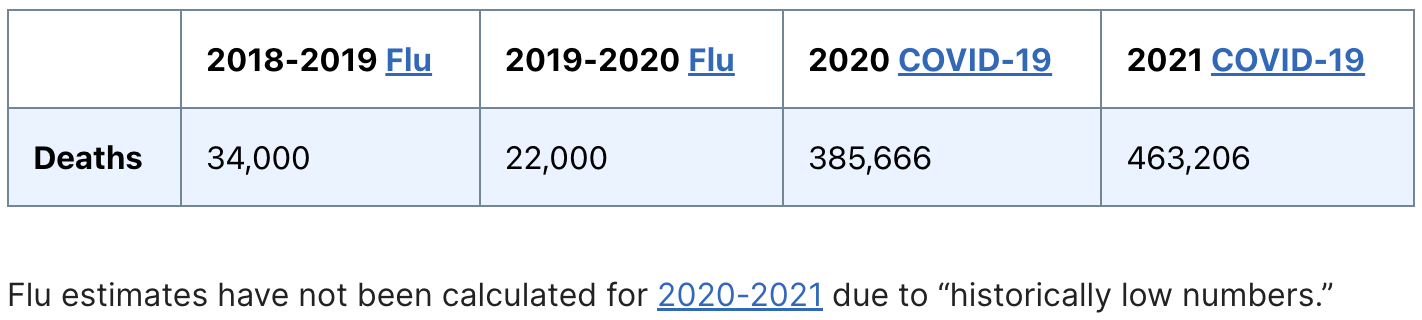
But thanks to vaccination and infection-induced immunity, Paxlovid, the use of corticosteroids (dexamethasone), and the evolution of the virus to prefer the upper airways rather than the lungs (thereby resulting in fewer cases of potentially deadly pneumonia), far fewer deaths are now resulting directly from acute Covid infections compared to two years ago.
So how deadly is Covid now compared to the flu? Here are the data from just the first two months of 2023:

Even now, deaths caused by Covid are outpacing deaths caused by the flu. The behavioral shift promoted by the world’s premier public health agencies to abandon virtually all protective measures against Covid is not based on the virus having burned itself out or attenuated its virulence to the point where it is no longer a threat to life and health. The pandemic is not over as Covid has not yet settled into a predictable pattern of seasonality or an acceptable level of disease and mortality that would qualify it as truly endemic.
Most concerning, in my view, is that SARS-CoV-2 continues to cause delayed onset health conditions at a very high rate compared to colds, flu, and other common viruses. For example, hypercoagulopathy (clotting) problems that can cause heart attacks and strokes, inflammation of the heart (myocarditis/pericarditis), and other cardiac and vascular conditions following even mild Covid infections have been well-documented and are almost certainly among the drivers of the ongoing elevated mortality rate seen all over the world, despite a declining mortality rate caused by acute Covid pneumonia.

And this seems to be happening at the highest rate among younger people. For example, recent data are showing a 33% increase in heart attacks following mild Covid infections among adults under the age of 45. What effect will CVD have on a young person’s life? How will it impact their longevity, work productivity, and quality of life (assuming that they survive)?
And while vaccination slightly lowers the risk of post-Covid conditions like strokes and heart attacks, the only certain way to avoid them is to not get infected in the first place. And for that, we probably need adjuvanted mucosal vaccines.
Last year, four countries (China, India, Russia, and Iran) rolled out their version of mucosal vaccines. Unfortunately, it is difficult to trust the information coming out of those countries, so we don't really know how many people have received mucosal vaccination or how those people are faring compared to unvaccinated individuals and those who were given traditional intramuscular vaccines. But it might not be a coincidence that China decided to finally end its lockdowns shortly after the rollout of its mucosal Covid vaccine…
Mosaic Vaccines
Adding an adjuvant is one way to improve vaccine effectiveness. Changing the delivery method from intramuscular to mucosal is another. And a third way is to create vaccines that are more broadly and durably effective by targeting the epitopes (areas) of the virus that don't seem to be mutating (evolving) much over time.
So far, the Covid vaccines have used the entire spike protein of SARS-CoV-2 as their immune target. And the result has been the production of a wide array of antibodies of differing clinical value, as some antibodies stick to parts of the spike that are not integral to the virus’s ability to cause infections while others do.
At the same time, key regions of the spike protein have shown themselves to be highly evolutionarily unstable with mutations taking place at a rate that would likely far outpace our ability to effectively roll out variant-specific updated vaccines, as we do with influenza. But there is one area of the spike protein that is both evolutionarily stable (i.e. it hasn't been mutating so far) and also critically important to the virus' goal of getting into our cells to cause infections.
The receptor binding domain (RBD) of the spike protein is the area in which the virus fuses with our cells' membranes as the first step in causing infections. Certain epitopes of the RBD have shown themselves to be genetically stable (conserved epitopes) and are found among all the variants of SARS-CoV-2.
Using nanoparticle technology, vaccinologists can now make vaccines comprised mainly of conserved epitopes. Such a vaccine would generate mainly antibodies that stick to the conserved epitopes of the virus' RBD and gumming up these epitopes would prevent cellular membrane fusion, thereby blocking infection.
Such a vaccine would look unlike any of the actual viral variants but would instead be comprised of just the clinically important and stable epitopes of all the important variants. Known as mosaic vaccines, several are currently in the works. They would generate memory B cells that would pump out powerful and evolutionarily durable antibodies. And, since many of the conserved epitopes on SARS-CoV-2 are also found on other human B coronaviruses, including certain viruses that cause colds, such a mosaic vaccine would likely offer protection that extends beyond Covid.
Better B Cells and T Cells
B cells that can latch onto multiple conserved RBD epitopes at the same time (strong-binding B cells) can make more effective (neutralizing) antibodies compared to weak-binding B cells that recognize just one conserved epitope. A mosaic vaccine could make stronger binding B Cells.

And, while the current vaccines rely mainly on training B cells to make antibodies against the spike protein, adaptive immunity also involves T cells which are capable of recognizing and targeting other of the virus' proteins, including the membrane (M) protein, the nucleocapsid (N) protein, and an area of the virus’ protein called Orf 3.
T cells capable of recognizing these other antigenic proteins can attack and destroy infected cells, killing the viruses inside them. A mosaic vaccine that contained epitopes from M, N, and Orf 3 proteins in addition to conserved epitopes of the RBD could provide stronger immunity, better mimicking that caused by natural infection.
An adjuvanted, mucosal, mosaic vaccine made using nanoparticle technology would engage the right immune compartment (the MALT), induce broad immunity against all the variants of SARS-CoV-2 (as well as some other B coronaviruses), and induce the strongest possible immune response, engaging B cells and T cells plus the innate arm of the immune system.
Caltech is currently testing a mosaic vaccine that combines epitopes from eight different variants of SARS-CoV-2 and the results look promising. And several other independent research labs are currently working on new vaccines with nearly 100 of them designed for mucosal (rather than intramuscular) delivery.
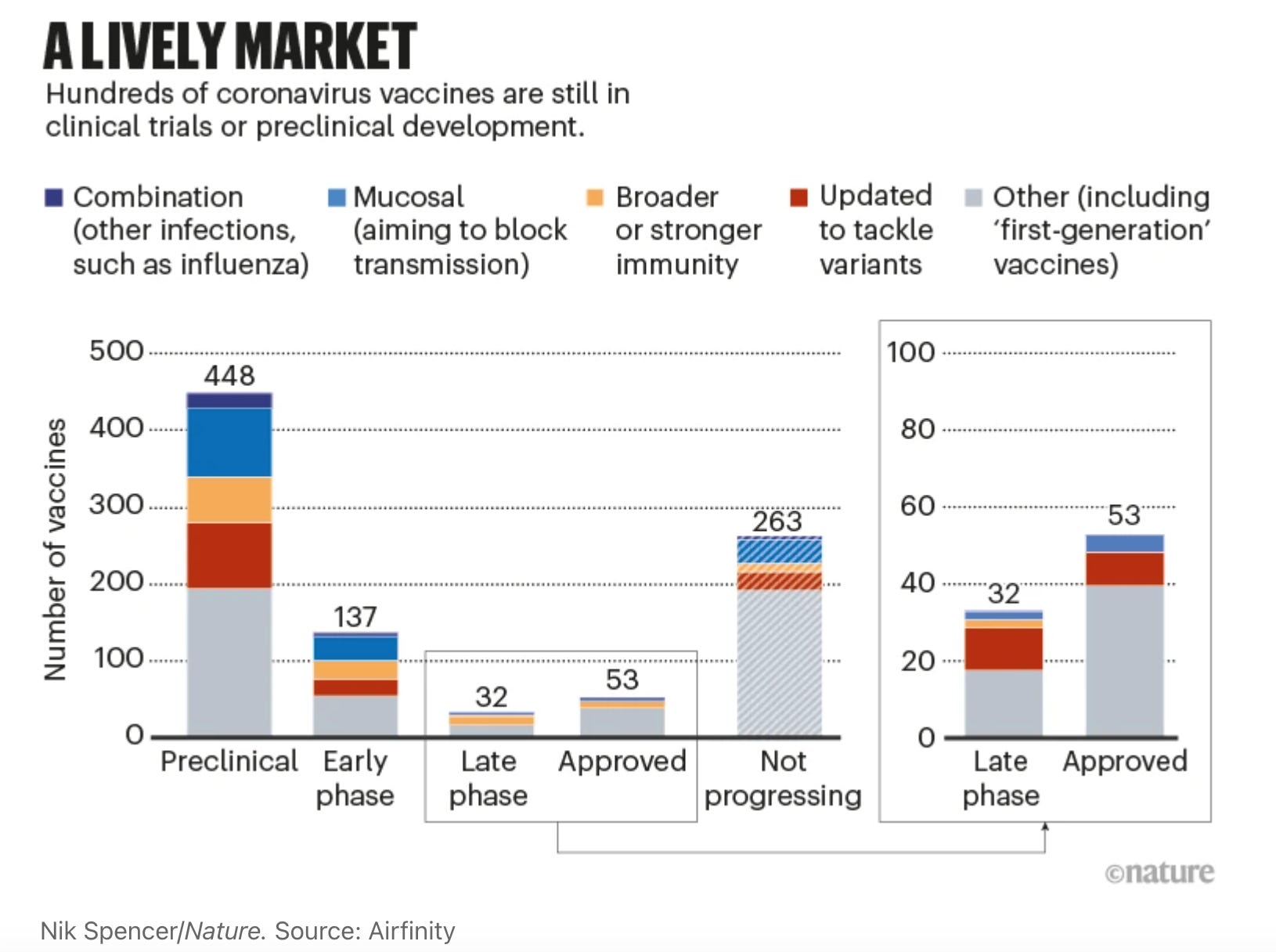
So there is a reasonable hope that better vaccines capable of preventing and spreading Covid are on the way, possibly this year, and that that would make a huge difference in terms of health outcomes by dramatically reducing the rate of both acute infections and serious post-Covid conditions. But the question is, will Americans take them?
Thanks to disinformation narratives falsely casting the Covid vaccines as dangerous–part of a conspiratorial effort involving big pharma, the science community, and governments around the world to constrain freedom–the US now has one of the lowest Covid vaccination rates and one of the highest Covid infection and mortality rates among industrialized countries. The effects of post-Covid conditions on the American healthcare system and workforce productivity have yet to be understood and the CDC (stunningly) does not seem to be too concerned about it.
When new vaccines that can help keep us much safer arrive, will we embrace them, or will the forces of disinformation whose aim is to erode faith and trust in science and medicine successfully undermine confidence in them as they have done with the Covid vaccines thus far? Will the CDC conduct a factually impeccable, apolitical, nuanced messaging campaign about the importance and limitations of the new vaccine(s) or will they again offer public health advice that is at odds with the most current data, willfully ignorant of long-Covid and post-Covid conditions, and rooted in doubling down on outdated historical practices, politics, and economics?