

COVID-19 Weekly Briefing for February 7, 2022

COVID-19 Weekly Briefing for Monday, February 7, 2022, in summary:
A review of the facts shows that a three-shot vaccination series is protective against infection, hospitalization, and death with Omicron; most adverse events reported after vaccination are due to nocebo; Omicron does not enter the cell via membrane fusion and has lower affinity for TMPRSS2-expressing cells (such as in the lungs and the olfactory nerve); the first C19 challenge study produces only upper respiratory disease–is this a sign that Omicron is spreading more through touch?; a review of BA.2; masks remain highly protective against Omicron; viral titers peak later with Omicron and remain high for longer as evidenced by persistently positive RATs between days 6-10; fourth shots of vaccine for immunocompromised; what measles can teach us about C19; a breakthrough in immunotherapy for cancer.
Just the facts, please...
1414 - 1420. Loose talk and casual narratives that get critical facts wrong about C19 can cause harm. Many influential people in the press and in public health have made statements recently suggesting, for example, that 'everyone' will likely become infected with Omicron, leading many to reasonably (but falsely) conclude that mitigation measures have become obsolete and we should go back to enjoying 'normal' life pleasures such as packing into bars, restaurants, concerts, etc., without any protective precautions.
Others have said that, because it is so hypertransmissible, anyone infected with Omicron will almost certainly pass it to everyone else in their home, leading many to reasonably (but falsely) conclude that isolating an infected member of the household is purposeless.
The CDC advises that fully vaccinated persons need not quarantine after exposure and may break isolation 5 days after being infected, without a negative test. Who thinks they know better than the CDC?
And others, pointing to the drop in vaccine effectiveness (VE) against infections with Omicron, even among fully vax'd (3-shots) persons, are promoting a narrative that the vaccines are no longer working, propping up and lending a patina of scientific credibility to an irrational anti-vax movement.
None of these ideas and recommendations are fact-based. And together, they serve to validate a misperception of hopelessness, exacerbating the sense of 'covid-fatigue' that most of us now share. For many of our patients, false narratives coming from experts are just the nudge they needed to give up on critically appropriate safety behaviors like isolating, quarantining, masking, testing, and avoiding the 'three C's.'
And this, in turn, is helping to drive case rates higher. Some doctors in our community are promoting falsehoods about vaccination. Many medical offices are still using surgical masks to protect themselves and allowing patients to wear cloth face coverings or none at all. One of my patients was told by her PCP that getting Omicron might be the best thing for her because it is 'just like getting a cold' and will provide her with 'better immunity than a vaccine."
We should continue to leverage our relationships of trust with our patients to counter disinformation, misinformation, and loose talk by sharing just the facts. So, what are the facts?:
The estimate of C19 prevalence during Omicron is that between 36-46% of Americans are likely to be/have been infected by Omicron by mid-February (when the wave is expected to be over). That means it is far from inevitable that 'everyone' will get it.

As presented in last week's briefing, the overall attack rate of Omicron within infected households is 31% (including fully, partially, and un-vax'd households). The secondary attack rate is significantly lower within fully vax'd (3-shots) households. Again, it is far from inevitable that just because someone in the household has C19, everyone will become infected. Isolation of infected members within the home remains a critical measure for breaking the chain of transmission.
https://www.medrxiv.org/content/10.1101/2021.12.27.21268278v1.full-text
Even though they were built 2 years ago against a variant that was substantially different from Omicron, fully vaccinated (3-shots) individuals currently have 50+% protection against infection, 90% against hospitalization, and 95% against death according to the least favorable data aggregates. If the first C19 vaccine arrived today with these levels of VE, it would be approved by the FDA and met with celebratory relief. This graph helps illustrate the point nicely:

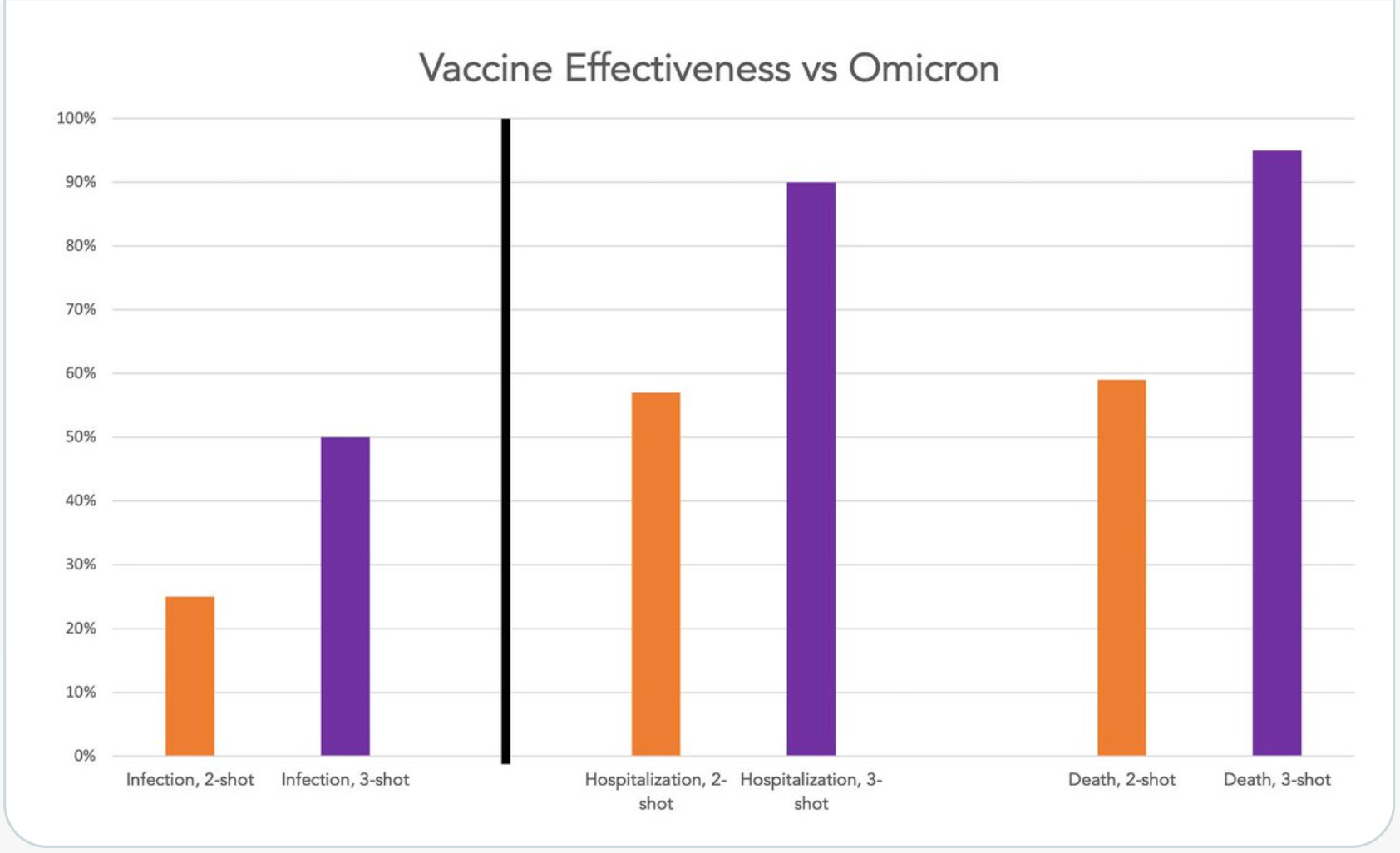
Of course, it is worth noting that if the vaccines were presented as a 2-shot regimen instead of 3, it would probably not get FDA approval since 2 shots offer only 25% protection against infection and the threshold for vaccine approval is, by convention, 50%. But the third shot (of mRNA vaccine) rescues and broadens neutralizing antibody titers to restore protection. We are promoting third shots to every patient who has not yet received one and should continue to do so.
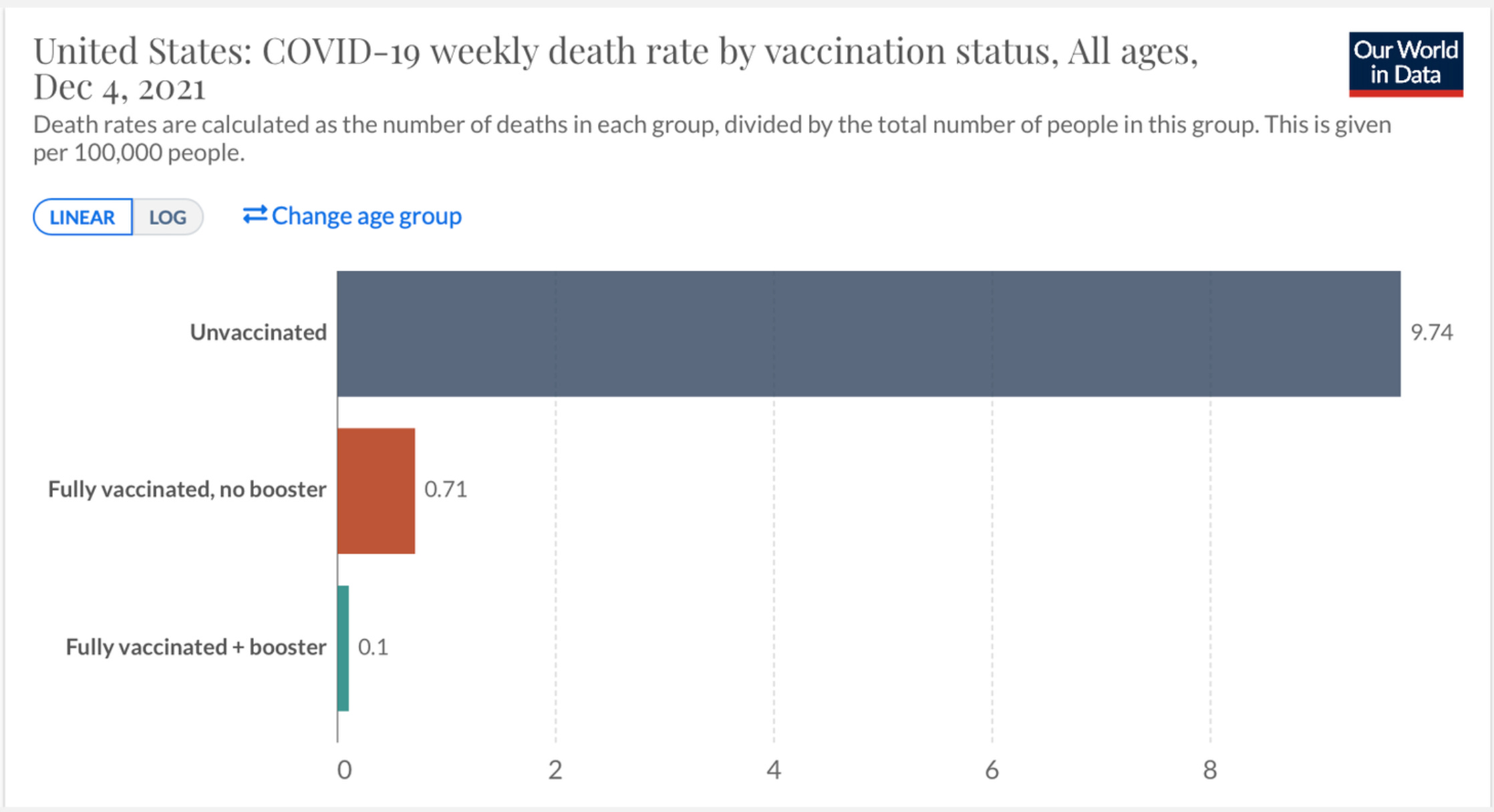
Here’s another way to look at VE: If you are unvaccinated, you are one hundred times as likely to die from C19 than if you are fully vaccinated (3-shots):
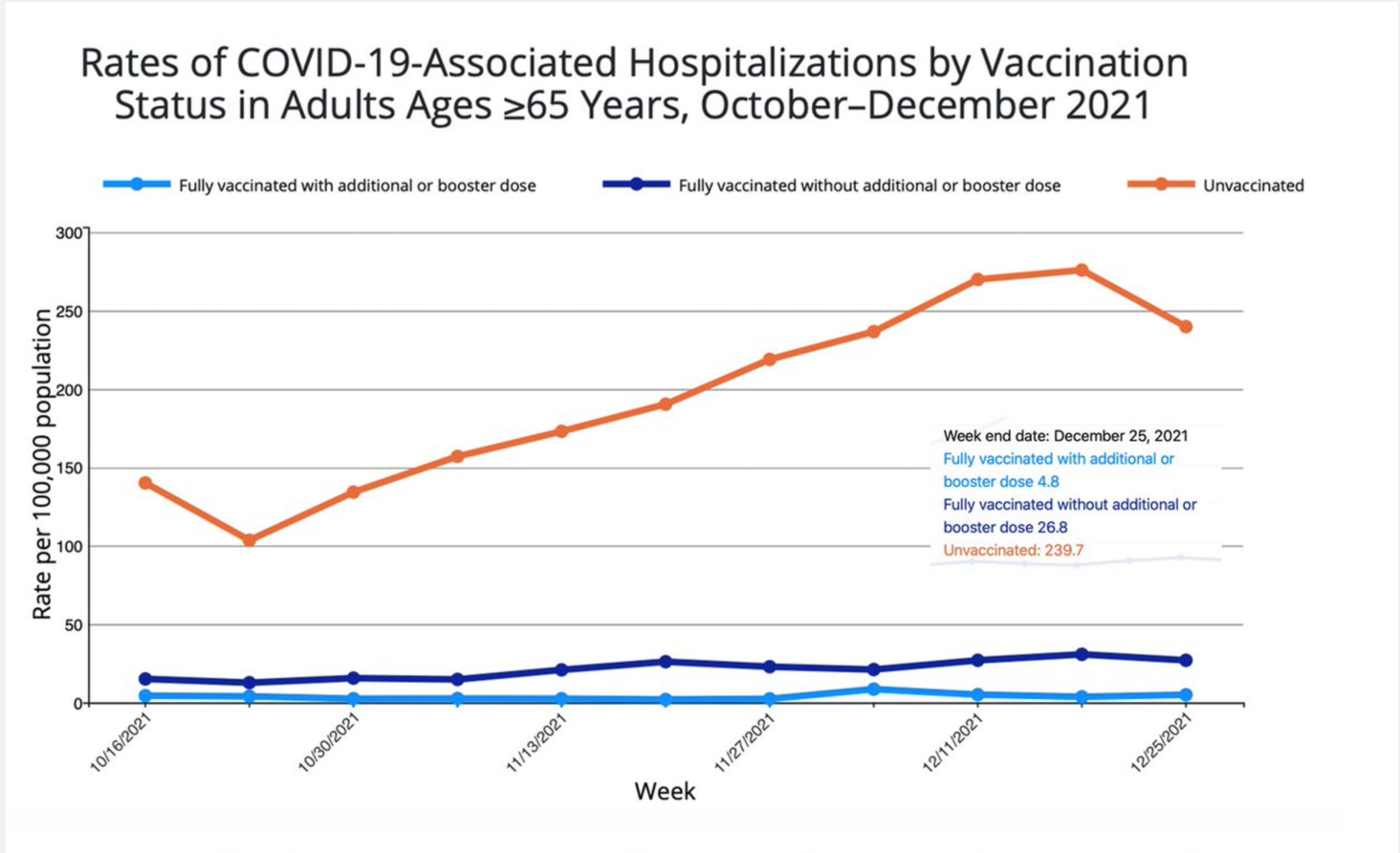
If you are 65 or older, you are more than 200 times as likely to be hospitalized compared to someone who is fully vaccinated (3-shots):
And, if you are under 65, you are about 80 times more likely to be hospitalized compared to someone who is fully vaccinated (3-shots):

According to the latest CDC data, fully vaccinated persons (3-shots) 65 and older are 98% protected against hospitalizations; 50-64YOs have 97% protection; and 18 - 50YOs have 96% protection compared to unvax'd.
We should be careful to set the tone with our patients using measured statements of fact that are dispassionate and anchored by the data. Here is how I have been reframing the false narratives about Omicron incidence, the value of isolating infected members within the home, and current vaccine efficacy being promoted in the press and among some medical professionals:
Current modeling predicts that between a third and a half of Americans will likely get C19 during the Omicron wave. That's based on the current (relatively low) level of compliance with expert recommendations to get three shots of vaccine, mask in public at all times, and avoid crowds. We can do much better by pulling together and complying fully with these recommendations. If we each do our part, we can keep Omicron from infecting three quarters of us but we all have to make some sacrifices for the good of our families, communities, and country.
There is a one in three chance of getting C19 from an infected member of your household. But that goes way down if you are fully vaccinated (3-shots) and much futher down if the infected person isolates properly. Infected persons should begin taking daily RATs on day 6 of isolation and come out of isolation only after two consecutive days of having tested negative (a minimum of 7 days of isolation). Once an infected person is able to end isolation, they should continue to properly mask around others at all times, indoors or outdoors, for one additional week. Far from inevitable, following this protocol will make transmission within the home highly unlikely.
It is truly astonishing that, two years after the vaccine was built, it is still so effective. Fully vax'd (3-shots) people have at least 50% protection against infections, 90% protection against severe illness, and 95% protection against death–even with the highly mutated Omicron variant. This is at least as good as the annual flu shot has historically been.
_____________________________________________
1421 - 1422. The nocebo effect accounted for 76% of reported systemic adverse events after the first dose of C19 vaccine, and for 52% after the second dose. Placebo effect = experiencing a positive/helpful/desired effect from something that could not possibly have caused such an effect (like a sugar pill or saline); nocebo effect = experiencing a negative/harmful/undesired effect, also known as an adverse event (AE) from something that could not possibly have caused such an effect. Many patients associate health changes that occurred in the period after vaccination with the vaccine itself and such reports can be found on VAERS. In most instances, this is the nocebo effect at work and not a true representation of vaccine-related AEs.
https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2788172
https://deutsch.medscape.com/artikelansicht/4910801
1423. The odds ratio (OR) for 3 doses of mRNA vaccine compared to unvaccinated gives estimated effectiveness at protecting against symptomatic infection of 67% for Omicron and 94% for Delta. OR for 3 doses v. 2 doses = 66% for Omicron and 85% for Delta.
Virology Update
1424-1425. Until Omicron, Scov2 infections proceeded as follows:
Attachment of the Scov2 spike receptor-binding domain (RBD) to ACE-2 expressed on the surface of human cells.
Cleavage of the spike protein at the junction between S1 and S2 utilizing TMPRSS2 to facilitate membrane fusion.
Introduction of the virus into the cell through the formation of syncytia following membrane fusion.
Omicron, because of its extensive spike mutations, including 15 mutations in the RBD, binds 3 times more strongly to ACE2 compared to Alpha or Delta but does not utilize TMPRSS2 efficiently and is less efficient at spike cleavage. These two factors impair viral membrane fusion which in turn makes viral induction into the cell/syncytia formation difficult.
Instead, Omicron enters human cells via fusion not with the cell membrane to form syncytia but via fusion with endosomal membranes–the way, for example, that nutrients enter cells. Omicron uses cathepsin (rather than TMPRSS2) for this process.
This study demonstrates that Omicron has less affinity for and replicates more slowly in cells known to express high levels of TMPRSS2 such as lung alveoli and lower airway and GI epithelia, but a high affinity for and high replication in cells known to express low levels of TMRSS2, such as trachea/upper airway epithelia.
In a nutshell, Omicron's high degree of RBD mutation has afforded it improved immune evasion properties at the expense of easy cell entry in TMPRSS2-expressing cells such as those found in the lower airways. This would explain the altered clinical picture with Omicron compared to prior variants, including significantly reduced ARDS (and therefore, reduced mortality). My note: If loss of smell during C19 is a function of neurotropism (nerve infection), the reduced reports of anosmia with Omicron could reflect the fact that TMPRSS2 is widely expressed by neuronal cells. High expression of TMPRSS2 in the olfactory nerve may act as a deterrent to neurotropism reflected clinically as lower rates of anosmia in Omicron. Extrapolating further, this could mean less CNS injury and perhaps less LC with Omicron compared to prior variants.
https://www.nature.com/articles/s41586-022-04474-x_reference.pdf
1426. The first human C19 challenge study has been completed. 36 volunteers aged 18-29 YO without evidence of previous infection or vaccination were inoculated with a low dose of wild-type Scov2 intranasally. Slightly over half became infected. Viral loads peaked 5 days post-inoculation. Virus was first detected in the throat but rose to significantly higher levels in the nose where it remained recoverable for up to 10 days post-inoculation, on average.
About 90% reported mild-to-moderate symptoms beginning 2-4 days post-inoculation. Anosmia developed in two-thirds of participants and persisted for > 6 months in several participants. Is this a sign of neurotropism and potential CNS infection/injury? No quantitative correlation was noted between viral load (VL) and symptoms, with high VLs seen across the board, including in those who had asymptomatic infections.
The world of science continues to refuse to broadly acknowledge the fact that long-term illness is common with C19 and delayed onset or chronic injury including the inducement of autoimmunity is, at the very least, a plausible outcome and serious concern for anyone who gets infected, regardless of the severity of the acute infection. Interestingly, none developed lower respiratory symptoms.
My note: Except for the high rate of anosmia, inoculation via intranasal drops with the wild-type strain produced a clinical picture that looked exactly like the one typically caused by Omicron. Is this an indication that Omicron is being spread via fomite transmission (inoculating the nose via touch)? Let's be sure to continue to wash our hands and disinfect objects.
https://www.researchsquare.com/article/rs-1121993/v1
Summary of Omicron (BA.1) vs. the new subvariant, BA.2
1427 - 1429. BA.1 = Omicron; BA.2 = the new subvariant of Omicron. BA2, which contains 27 distinct new mutations not seen in BA1, now accounts for the majority of cases in India and Denmark and is steadily on the rise, outcompeting BA1 in South Africa, Sweden, Singapore, and elsewhere. It has been identified in 57 countries including the US.
The WHO has decided to treat all Omicron sub-lineages as one VOC and has not assigned BA.2 its own Greek letter (I don’t understand why but suspect they are concerned about running out of Greek letters and having to create another entirely new nomenclature system).
Early data from Denmark show that BA.2 spreads (within households) 30% faster compared to BA.1 and has more immune evasion. In theory, this could lower vaccine-induced protection but data from the UK shows vaccine effectiveness against symptomatic infection to be slightly better against BA.2 compared to BA.1. Specifically, protection against BA.2 after two and three shots was 13% and 70%, respectively, while against BA.1 it was 9% and 63%, respectively. Clinically, it does not appear that BA.2 is more virulent and it may even be less virulent compared to B.1.
In Denmark, for example, despite cases and hospitalizations reaching pandemic record levels, ICU admissions are plummeting.

As societies reach a version of herd immunity and new variants undergo selective pressure toward immune evasion, we should expect that ever higher degrees of mutation will inform the virus' transmission and replication dynamics as well as its clinical expression. Omicron, because of its highly mutated RBD, is having trouble using TMPRSS2 and cleaving its spike protein to achieve cell membrane fusion. That has lowered its affinity for high TMPRSS2-expressing cells such as those in the lower airways and the olfactory nerve, altering the clinical picture to look more like a cold than pneumonia or 'classic covid.' BA.2 looks, by early reports, to produce the same pattern of illness and perhaps even be slightly less virulent than Omicron (BA.1).
Masking and testing to break the chain of transmission
1430. An update on the effectiveness of masks: a case-control study from the CDC MMWR shows that for indoor gatherings, the use of masks reduced infections by >60% and there was a substantial increase with higher quality masks to >80%. Masking efficacy is probably much higher still if high-quality masks are also properly fit to the face with no air gaps.
Among those who report always wearing cloth, surgical, or high-efficiency masks in indoor public settings, the odds of infection were reduced 56%, 66%, and 83%, respectively, compared to those who did not always wear masks in indoor public settings.

https://www.cdc.gov/mmwr/volumes/71/wr/mm7106e1.htm?s_cid=mm7106e1_w
1431. Over the first 2 weeks of January, 43% of 260 healthcare workers (HCWs) on days 5-10 of symptomatic illness who felt sufficiently recovered to return to work had positive RATs between days 5-10, including 26% of those who returned on days 8 and 9.
HCWs who tested positive on their first test most often remained positive on their second test (56%). HCWs with three shots were nearly twice as likely to test positive during this period and nearly 3x as likely to test positive on day 5.
These results indicate that a substantial proportion of people with C19 are likely still contagious after day 5 of illness regardless of symptom status. My note: Why are fully vax'd (3-shots) people testing positive for longer? They're not, actually. They are testing positive later. They are symptomatic earlier (immune symptoms such as runny nose, sore throat, sneezing, congestion, fever, etc.) which leads to earlier diagnosis which shifts the testing window to the right.
Second note: In the past, RATs had a very narrow testing window of 1-2 days. That was before most people had strong prior immunity and symptom onset was often on day 5, 6, or 7, when viral titers were already at their peak and symptoms were from viral injury (fatigue, brain fog, difficulty breathing, cough). The authors conclude: "Early liberation from isolation should be undertaken only with the understanding that inclusion of individuals on day 6-10 of illness in community or work settings may increase the risk of COVID-19 spread to others which, in turn, may undermine the intended benefits to staffing by resulting in more sick workers." I would add that, in the long-term, such “early liberation” might also increase the number of people who go on to LC and delayed-onset illness and disability.
https://www.medrxiv.org/content/10.1101/2022.02.01.22269931v1.full.pdf
Patients are asking about 4th shots
1432 - 1435. The Washington Post reports that the CDC now recommends immunocompromised patients get a 4th shot and that J&J for immunocompromised be updated to a 2-shots primary regimen with a booster recommended 2 months later. This has not yet appeared on the website, however. Should all adults be getting a 4th shot as they are now doing in Israel? The Israeli data originally reported through leaks were mostly disappointing. But now that the data have been released we can see that among those 60 and older, a 4th shot improves protection against severe disease 3 to 5-fold. It boosts antibodies in all age groups well beyond the levels seen after the third shot too, which might, at least in theory, offer some extra protection against infection. But will it and if so, for how long? At this time, our office should allow 4th shots with provider approval only, with the understanding that the designation of 'immunocompromised' is a question of clinical judgment.
https://www.washingtonpost.com/health/2022/02/04/coronavirus-booster-shots-immunocompromised/

In a nutshell, the actual Israeli data, contrary to early reports, support fourth shots–at least for immunocompromised patients, issues of politics and equity aside.
https://www.medrxiv.org/content/10.1101/2022.02.01.22270232v1.full.pdf
Covid Adjacent
1436 - 1437. Fascinating article summarizing Michael Mina's work on measles and the effect of morbillivirus on post-infection immune function. Here are the key big-picture data:
Measles causes suppression of immunity x approximately 1 month, during which patients tend to feel quite sick.
After resolution and general restoration of immune function, patients who survive measles become highly susceptible to other infectious diseases, including those against which they had prior immunity through either prior infections or vaccinations.
This, in turn, translates to a 5-fold increase in mortality rate from infectious diseases among measles survivors compared to uninfected.
As it turns out, morbillivirus not only temporarily suppresses generalized immunity, it specifically destroys plasma cells (specialized B cells that have been primed to pump out extremely high amounts of a particular antibody against a particular pathogen). By destroying these plasma cells, morbillivirus can reduce circulating antibody titers by as much as 70%, wiping out large swaths of prior immunity, a phenomenon known as 'immune amnesia,' leaving survivors vulnerable to a host of infectious pathogens against which they had had protection prior to getting measles. Measles, according to Dr. Mina, may be implicated in as many as half of all childhood infectious disease deaths.
It took more than 100 years for science to put together the pieces of this stunning story. What will we learn about Scov2–a virus that we already know causes chronic illness and multi-organ damage including immune system dysregulation? Will C19 drive up the incidences of autoimmunity and related diseases such as RA, lupus, EBV, MS, and others? Will it make survivors more susceptible to other infectious illnesses? We don't know for sure but the data (already large and building by the day) are telling an early story that is not optimistic.
To those now advocating for treating C19 as we do colds and flu, we should provide this reminder that the data strongly suggest that many people who get infected will not be moving forward to as healthy or as long a life as they would otherwise have had had they managed to avoid getting infected.
https://medicalrepublic.com.au/the-great-measles-immunity-heist/25264
Non-Covid
1438. A major breakthrough in cancer therapy: CAR-T cell therapy involves removing T cells from a person with cancer, genetically altering them so that they produce proteins called chimeric antigen receptors (CARs) that recognize cancer cells, and then reinfusing them into the patient in the hope that they will seek out and destroy cancer tumors. It now appears that, over time, patients who receive CAR-T cell therapy develop CD4 T cells that know how to kill the cancer cells, and these CD4 cells are retained. There are now two terminal patients with CLL who were treated with CAR-T cell therapy and are 10 years cancer-free. Possible other uses for CAR-T cell therapy include difficult-to-treat infections.