

COVID-19 Weekly Briefing for Monday, January 17, 2022

Dear LJVFMG Team,
Happy MLK Day. I hope everyone has a chance to enjoy their day off today and perhaps to reflect a bit on this particular holiday. Growing up in New York at a time when racial integration of schools and neighborhoods was first being advanced as the articulated goal of national political leadership, polarizing the nation, the tendrils of Dr. King's message of justice reached my community, my school, and my family. It was discussed and debated in the classroom, on the playground, and at the dinner table, substantially shaping my image of what America might become if only, individually and collectively, we were willing to take moral responsibility for the contradictory impulses of our own hearts.
We are all selfish and generous, suspicious and kind, judgmental and forgiving. Dr. King–perhaps better than any person in recorded history–explained in language at once plain and poetic, why choosing the better angels of our nature was in the interest not only of our national soul but our individual souls. He pleaded, at that critical moment in our history, for each person to man an oar and pull together toward the American dream of justice for all and affirm our identity as a people bound not by race or ethnicity but by an idea whose realization required only our willingness to summon the courage to fight for fairness, dignity, and decency–endpoints that seem as self-evidently correct and imperative to me at sixty as they did at six.
____________________________________________________
This week's briefing begins with a discussion of what we know so far about Omicron including its clinical presentation, incubation and infectious periods, as well as how and when to test and which tests to use.
C19 Symptoms and their timing in the time of Omicron
1357 - 1362. Congestion, runny nose, sneezing, and fever are all symptoms of immune system activation. Vasodilation and initiation of mucous secretion (congestion and runny nose) help to wash away pathogens, while high-velocity expulsions of air (sneezing) help eject them and fever creates a too-hot environment for them to thrive. These are some of the mechanisms used by our immune system to get battle viruses like SARS-CoV-2 (Scov2).
By contrast, loss of smell/taste (anosmia/ageusia), shortness of breath (SOB), and brain fog are symptoms of injury to bodily tissues caused by the virus.
Cough can be either an immune response (the activation of laryngeal, esophageal, or tracheobronchial receptors when viral infection of airway epithelia stimulates the immune system to release cytokines or secrete airway mucous to trigger the cough response) or it can be induced by highly pathogenic viruses when they attack infected cells in the lungs or airways–the body's attempt to slough off and expel dead tissue. The same is true of sore throats which can be caused by vasodilation and swelling as an immune response (as seen in both colds and allergies) or by viral injury when an infection is centered there to cause significant tissue damage (as seen in strep throat and influenza).
Vaccination trains our immune system to recognize specific pathogens and quickly initiate immune responses to combat them. Prior infection also creates this kind of prior immunity and when a person’s defenses are primed for battle, symptoms can start as early as a couple of days after an infection. But if a person has no prior immunity, it can take more several days before the immune response builds to the point of become a symptom.
At the beginning of the pandemic when none of us had prior immunity to Scov2, loss of smell/taste, cough, and shortness of breath (SOB) were consistently among the first symptoms of COVID-19 (C19). They would typically appear 5-7 days post-exposure–a fairly long incubation time–after enough virus had built up and caused sufficient viral injury to result in symptoms. There were fewer immune symptoms at that time because our symptoms had not been primed. Pneumonia was common then, as the early Scov2 variants tended to center infection in the lungs. Early C19 was described as a characteristically dry, mostly lower airway disease.
Now, with most people having prior immunity from vaccinations and previous infections, and with the current variant (Omicron) centering infection in the upper airways (nose and throat) rather than the lower airways (lungs), we are seeing the onset of immunity symptoms (runny nose, congestion, fever, sneezing) within 2-3 days of exposure (shorter incubation) followed with a far lower percentage of cases progressing to symptoms of viral injury compared to prior variants.
This is the silver lining to the Omicron cloud. For example, according to the ZOE project, the top 5 symptoms of Omicron are:
Fatigue
Sore throat
Runny nose
Sneezing
Headache
Anosmia, seen at a rate of 80+% during the Alpha wave, is occurring in only about 19% of Omicron cases; brain fog is at just 24%; and SOB, once a dominant feature of C19, is no longer even making the list of the top 20 symptoms since Omicron took over.
In most cases, those of us with primed immune systems–especially those of us with three shots of vaccine or two shots of vaccine plus a prior infection–are preventing the progression of C19 to severe disease. This is further helped by the fact that Omicron replicates more slowly in the lungs compared to Delta and other prior variants.
The Timing of C19 Infectiousness During Omicron
In addition to the above, in this conversation between Michael Mina and Andy Slavitt, we learn that infectiousness is not correlated to symptoms. People can spread the virus regardless of how sick they feel (or whether or not they feel sick). This applies also to waning symptoms which, as Mina points out, is not a trustworthy indicator of non-infectiousness.
With Omicron, the average time to peak of viral titers (and therefore, it is widely assumed, to the peak of infectiousness) is 5 days from exposure. Those with stronger prior immunity (3 shots or 2 shots plus prior infection) may take more than five days to reach the peak of viral titers as immunity slows the virus’ progress. That means that for people with prior immunity, onset of symptoms (OOS) often precedes infectiousness by at least 2-3 days. It also means that testing during the first 1-2 days of symptoms, before viral titers have had a chance to reach their peak levels, is less reliable, especially when using rapid antigen tests (RATs) which are only sensitive when viral titers are near or at their peak. For those with prior immunity, we should expect false negative results during the first 1-3 days of symptoms. We should also expect that RATs will remain positive well beyond day 5 of symptoms, especially among those with stronger prior immunity who might have delayed time to peak viral titers. Such patients should be expected to have high viral titers later in the disease course and therefore, to be infectious more than 5 days post-OOS regardless of whether symptoms are worsening, improving, or nonexistent.
By contrast, those without any prior immunity and some with lower prior immunity (2 shots or less) will not develop up-front immune symptoms as quickly, leading to longer incubation times similar to those seen with prior variants like Alpha. These people will be more likely to have presenting symptoms of viral injury such as anosmia/ageusia, brain fog, profound fatigue, and cough with or without shortness of breath, typically beginning on day 5 post-exposure. Those with low or no prior immunity are likely to begin testing positive on the first or second day of symptoms and will be less likely to continue to test positive on RATs after 5 days of symptoms.
Clinically, this informs our testing recommendations and interpretation. Viral loads and infectiousness are more closely linked to symptoms among under-immunized/unimmunized patients but are uncoupled among those with strong prior immunity.
Mina also confirms that infected people may start spreading Omicron as soon as one or two days after exposure/infection. With a replication rate estimated at 70x faster than Delta in the bronchi, we can reasonably assume that airborne virus is being emitted through breath and speech very soon after infection. Among immune naive/underimmune, with a longer incubation period, infectiousness is, therefore, likely to precede OOS by 3-4 days on average, creating a longer pre-symptomatic period among unvaccinated people that is particularly dangerous.
My note: This is likely one component of Omicron's astoundingly high level of contagiousness. A higher degree of immune evasion because of the number of new mutations is another. And the wet upper airway disease (runny nose and congestion) is likely another. Omicron is probably resulting in much higher levels of fomite transmission (infections spread through touch) compared to prior variants. Sneezing and runny/stuffy nose means nose blowing and rubbing which transfers virus to the hand of the infected and then the doorknobs, keypads, and other communal survaces that they touch. Someone else touching those surfaces can then transmit the virus to themselves when they touch their eyes, nose, or mouth. For this reason, handwashing and surface decontamination which were prioritized by the CDC as the chief behavioral mitigation measures at the beginning of the pandemic (when, because C19 was a 'dry' illness, was probably not an effective means of reducing transmission) has become far more important with Omicron. Ironically now, with the arrival of Omicron, the CDC is finally shoring up their message about wearing high-efficiency masks.
C19 Testing and Timing During Omicron
1. Lab-based PCR: With regard to testing, Michael Mina confirms that Omicron starts in the throat/oral pharynx and then progresses toward the nose later in the disease course making all testing less sensitive if nasal swabs alone are performed at or near the peak of viral titers (around 5 days post-exposure). Lab-based PCR is the most sensitive test. It can catch the infection as early as 2-3 days after exposure and stay positive for 3-4 weeks as it detects nucleic acids present in viral debris that can sometimes takes a long time to clear (not new data). But patients with more prior immunity who mount strong up-front immune defenses can sometimes battle the virus' colonization of the airways with enough success to suppress viral titers, delaying a positive test for a few days. My note: Best practice should include factoring prior immunity into our testing strategy. A boosted patient (3 shots) with an exposure who develops a runny nose or other cold-like symptoms and tests negative by lab-based PCR on days 1, 2, or 3 of symptoms, should continue to take RATs daily for at least 4 more days (until day 7 post-OOS) unless or until they get a positive test before breaking isolation. These patients should exercise extreme behavioral caution (isolation is best) until at least day 7 of symptoms and have two consecutive negative RATs, the first of which should be on or after day 6 of symptoms, before assuming they are safe to be around others again or before attributing their symptoms to other than C19.
2. 'Rapid PCR' tests: We also learn that the so-called 'rapid PCR' tests are not actually PCR tests; they are lateral flow molecular LAMP assays that are only slightly more sensitive than RATs and less sensitive than actual (lab-based) PCR tests. From the FDA:
The SARS-CoV-2 RT-LAMP Diagnostic Assay is a loop-mediated isothermal amplification (LAMP) assay designed to detect nucleic acid from Scov2 in nasopharyngeal swabs, oropharyngeal swabs, anterior nasal swabs, mid- turbinate nasal swabs, nasopharyngeal washes/aspirates or nasal aspirates.
Whereas a lab-based PCR test in an unvaccinated or under-immunized person can reasonably be expected to turn positive on day 3 or 4 post-exposure, a LAMP assay test should be expected to turn positive 24 hours later, on day 4 or 5, while a RAT should be expected to turn positive 12 hours later than LAMP, on day 4.5 or 5.5 (if performed correctly using a throat plus a nose swab). That means the so-called 'rapid PCR' tests being offered for $200-$300 per test here in San Diego provide only about 12 hours earlier detection compared to a RAT. That hardly seems worth the cost. In addition, LAMP tests should not be performed in the cold, so the so-called 'rapid PCR' tests being conducted at outdoor field testing sites will not provide accurate results in cold weather.
3. Rapid Antigen Tests: Because RATs are typically only positive during the period of peak viral titers, the best days to test unvaccinated or under-immunized patients are days 5, 6, and 7 post-exposure or days 1, 2, and 3 of symptoms. The best days to test patients with strong prior immunity (three shots or two shots plus a prior infection) are days 4, 5, and 6 of symptoms or days 6, 7, and 8 post-exposure. In all cases, RATs should be used on consecutive days unless and until they return a positive finding. Because they are only positive at the peak of viral titers, positive RATs have a 90+% concordance with infectiousness. However, negative RATs do not have high concordance with a lack of infectiousness. RATs are most accurate when timed properly and when tests are performed in the middle of the day (when viral titers tend to be highest). If negative, they should be performed for several days in a row (at least three sequential days, properly timed is ideal) using the combined throat and nasal swab technique.
The other use for RATs is to help break quarantine/isolation. Negative RATs two days in a row, beginning on day 11 post-exposure or day 6 post-OOS among unvaccinated/under-immunized patients is reasonable for ending quarantine/isolation. Negative RATs two days in a row beginning on day 12 post-exposure or day 7 post-OOS among fully immunized patients is also reasonable.
Finally, with regard to RAT brands, Quidel's RAT has more false positives compared to Binax Now (1/150 vs. 1/3,000). It is also slightly less sensitive. That does not invalidate Quidel but we are trying to source Binax Now and other brands here at the office.
Summary of Testing: Now that access to PCR tests is reduced and because PCR tests can continue to detect viral nucleic acids in post-infection debris for up to a few weeks, we our office’s 'back to work' protocol will consiste of 2 consecutive days of negative RATs following 5 days of isolation. This means that at our office, a minimum of 7 days isolation including two consecutive days of negative RATs taken on days 6 and 7 or 10 days isolation with a single negative RAT on day 10, are required for return to in-office patient care.
We should dissuade patients from seeking so-called 'rapid PCR' tests which offer only slightly better sensitivity than RATs, are expensive, and are unreliable if performed in cold weather. Remember, RATs should be performed using a combined throat and nose swab, ideally during the middle of the day.
___________________________________________
Paxlovid Update
Paxlovid is an Mpro-directed therapy. It targets and inhibits the virus' main protease (SARS-CoV-2-3CL)–an enzyme that the virus needs to replicate. This quickly reduces viral load 10-fold thereby inhibiting transmission as well as progression of the illness. The portion of Scov2 targeted by Paxlovid has had extremely high genetic retention (only 1 mutation in that region of the virus since it was first identified > 2 yrs ago). That implies that it should continue to be effective against new variants unless we see a sudden antigenic shift of that region for the first time.
The rate-limiting step in its manufacturing is the raw materials that are sourced chiefly in China. Bangladesh and India are now making generic versions. The 80M promised domestic doses will not be nearly enough to move us to phase III of the pandemic in which we are able to establish an acceptable new normal. My take: we need a new Operation Warp Speed-type program to manufacture high-quality masks, rapid tests, and Paxlovid. Paxlovid should be made in both pill and nasal spray forms. It should be in every purse, backpack, and medicine cabinet and started immediately after exposure or upon the earliest onset of symptoms.
1363. 500 doses of Paxlovid arrive at family health centers in San Diego but it's a pittance with tens of thousands of daily cases here. Small amounts are also available in pharmacies. Unvaccinated are prioritized over vaccinated, older and immune-vulnerable over younger and immune-competent.
1364. However, at the current pace, it may take months before Paxlovid can be widely distributed.
https://www.washingtonpost.com/health/2022/01/04/antiviral-pills-supply-omicron/
Epidemiology Update
1365. It looks like the high amplitude/short duration Omicron spike that we saw in South Africa may be happening elsewhere.
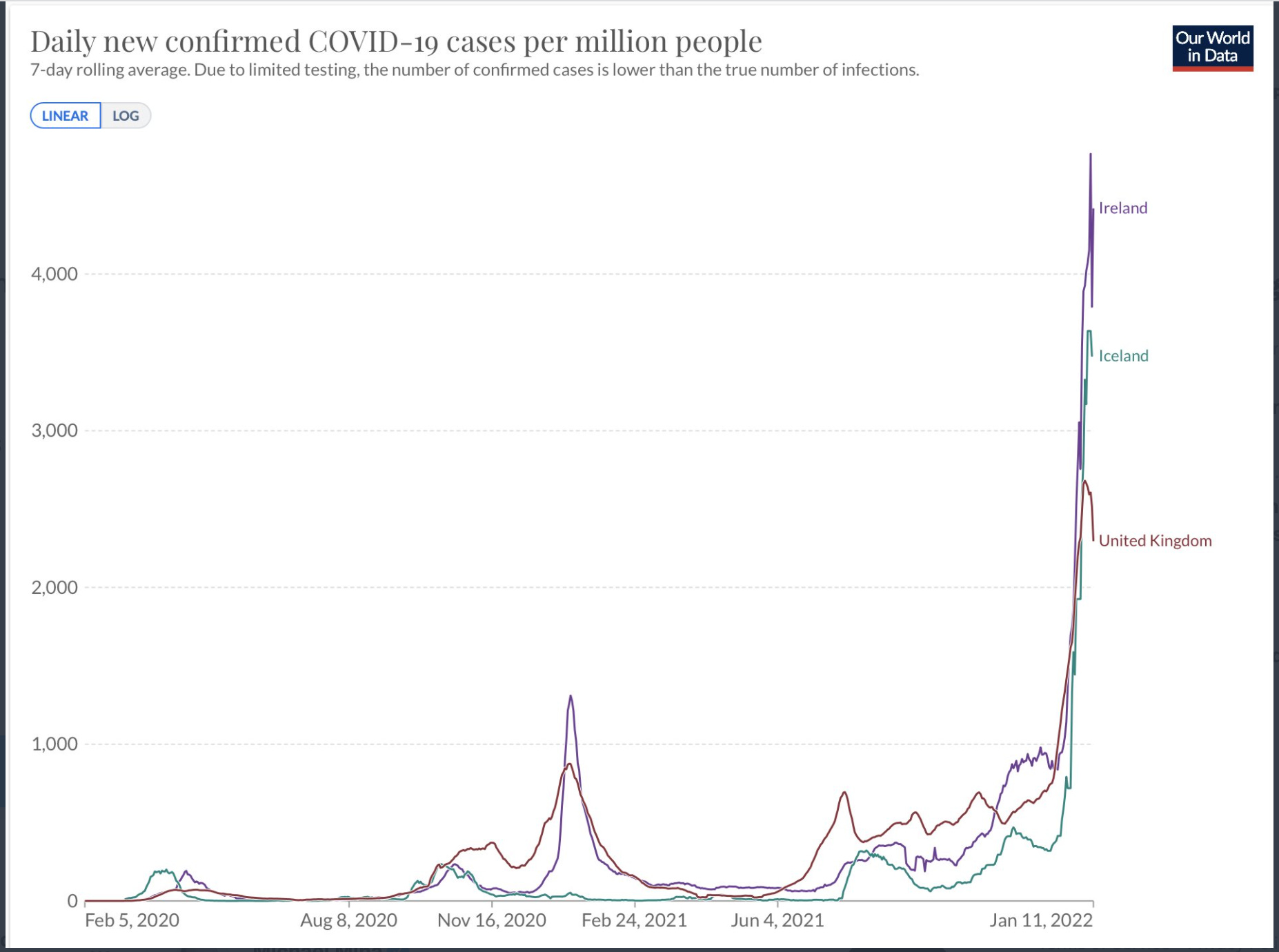
Let's hope we see the same in the US which is, as yet, showing no signs of having peaked.

https://ourworldindata.org/coronavirus/country/united-states
1366. San Diego had a record-breaking 52K cases reported in one day yesterday (1/11/22). Some of this is likely a carryover from last weekend, but even still, the average daily rate is 14K and we should view this as only about 1/4 - 1/5 of the true case numbers for reasons previously discussed.
https://www.nytimes.com/interactive/2021/us/san-diego-california-covid-cases.html
1367. On the plus side, there should be no question now that Omicron is less intrinsically virulent compared to prior variants. Slower replication in the lungs is leading to far less ARDS as reflected in the low ICU/CCU rates compared to Delta in this study from Kaiser Foundation in Southern California where Delta and Omicron cases (distinguished by the presence or absence of SGTF on PCR testing) were compared concurrently from Nov through the beginning of January:

https://www.medrxiv.org/content/10.1101/2022.01.11.22269045v1
1368. However, along with the decreased rate of severe disease/death, there is a significantly increased rate of cases and this is leading to overall high rates of hospitalizations in areas hit hardest. For example, here are the hospitalization rates in Florida over the last 3 months; take particular note of the last 3 weeks since Omicron took over:

So, yes, any individual who gets Omicron is less likely to wind up hospitalized. But so many people are getting infected that hospitalizations are going up anyway, almost everywhere.
https://www.nytimes.com/interactive/2021/us/florida-covid-cases.html
1369. In San Diego, we have seen a 17% increase in hospitalizations over the last week.
https://sdcounty.maps.arcgis.com/apps/dashboards/30b5e0fa2a5f4404b1219d8cd16b2583
Long-Covid Update
***1370. C19-related anosmia is associated with viral persistence and inflammation in human olfactory epithelium and brain infection in hamsters. Residual Scov2 viral antigens have also been detected in GI and hepatic tissues from recovered patients with C19. In this fascinating study, underarm samples were self-collected by 45 patients with long-covid (up to 1.5 years post-infection) and 188 controls who were asymptomatic with negative PCR tests (people who did not have long-covid and were not currently acutely infected). Dogs trained to detect specific volatile organic compounds (VOCs) triggered by Scov2 infection correctly identified 23/45 samples taken from long-covid patients versus 0/188 controls, suggesting persistent viral presence in some patients with long-covid. Is long-covid an ongoing immune reaction to the retention of Scov2 antigen in various previously infected tissues or even an ongoing infection?
https://www.medrxiv.org/content/10.1101/2022.01.11.21268036v1
1371. In this amazingly well-done study comparing patients with long-covid against those who had fully recovered from C19 and those who had not been infected by Scov2, as well as those who had been infected by other human coronaviruses (including cold viruses), we see components of the acute inflammatory response (especially interferons Alpha and Beta) and activation of fibroblasts, epithelial cells, T cells and myeloid cells associated with only the long-covid group at 8 months post-infection. There was a chronic activation of a subset of CD8 T cells (killer T cells) and monocytes persistent at 8 months in only the long-covid cohort as well as an absence of naive T and B cell subsets in just this group, suggesting that Scov2 infection exerts unique prolonged residual effects on innate and adaptive immunity which could be driving the fatigue, headache, and persistent cough associated with long-covid. My take: The authors also hypothesize that SOB, brain fog, and other long-covid symptoms might also be caused by persistent immune dysregulation but such symptoms (as well as anosmia) are symptoms of viral injury which suggest to me permanent alterations of lung and brain tissues.
https://www.nature.com/articles/s41590-021-01113-x
1372. Long-covid 'brain fog' (impairment in attention, concentration, speed of information processing, and memory) is strikingly similar to cancer therapy-related cognitive impairment (CRCI). This study looked at human brain tissue, CSF aspirates, and mice to demonstrate that even mild C19 infections cause the same pattern of neuroinflammation as is seen after chemotherapy: microglial reactivity, pro-inflammatory CSF cytokines/chemokines including CCL11 (which is associated with impairments in neurogenesis and cognitive function) resulting in impaired hippocampal neurogenesis, decreased oligodendrocytes, and myelin loss in subcortical white matter in mice. These are all things seen commonly in CRCI. They did not look at neurotropism (direct infection of nerve/brain tissue) which has been hypothesized to be the cause of grey matter destruction seen on pre and post C19 MRI studies (remember the UK biobank study).
https://www.biorxiv.org/content/10.1101/2022.01.07.475453v1.full
1373. The risk of developing long-covid is cut in half by vaccination (pre-Omicron study). Will this be true with Omicron infections? Will Omicron cause more long-covid because it is more immune evasive or less because it is less likely to progress to viral injury? No one knows for sure so we should be erring on the side of caution and continue to advise our patients to take the right steps to avoid infections.
https://www.sciencedirect.com/science/article/pii/S1473309921004606
Mask Update
1374. Comparing N95 respirators with and without nose bridge adjustment bars against surgical masks, this very detailed study shows that the more perfect the fit of the mask, the more protection you get. Using a typical Scov2 viral load and infectious dose, social distancing at 10 feet indoors between two speaking individuals leads to a 90% risk of infection (ROI) after a few minutes. If only the susceptible wears a face mask with the infectious person speaking from a distance of 5 feet it could take 30 mins to reach 90% ROI and with a properly fit N95, the ROI after an hour is only 20%. If both wear a surgical mask, the ROI is 30% after 1 hour. If both wear well-fitted N95, it drops to just 0.4%. Bottom line: in this modeling study, masks are protective but distancing is not and high-efficiency masks, if worn properly by both parties with no face gaps, can reduce ROI in our exam rooms to almost zero. This is what we have been doing since March, 2020, using our wonderful KF 94 masks from Korea.

We should take this with a grain of salt, remembering that it is a modeling study. We should also assume that protection would be significantly lower if we were subjected to close, prolonged exposure to an unmasked infected person, even if we were masked. Patients must not be allowed to remove their masks inside our office and especially not in the exam rooms. We should follow our established protocol of using the hand-held fan directed at the face of patients, seated in front of a fully open window, on the rare occasions when we must look into their mouths or noses.
https://www.pnas.org/content/118/49/e2110117118
Vaccination Update
1375 - 1376. As I have said several times, fully vaccinated should = 3 shots (like many other vaccines) whether the FDA and CDC are willing to say so or not:

And we may need an annual booster (4th shot) if a more effective, pan-beta coronavirus vaccines has not been made available (hopefully as an oral or nasal spray preparation) this year. This is not unusual! Polio follows a standard 3-shot primary regimen with a fourth shot (booster) and DTaP follows a standard 3-shot primary regimen with two boosters for a total of 5 shots. What is different is the current timing of booster shots–at least with regard to the 4th shots being given currently in Israel. Is this the correct and appropriate response in the midst of a pandemic or is it too many shots too close together to be maximally effective? There are no compelling data that I'm aware of to argue the case either way so the current WHO and EMA arguments against fourth shots are based on expert guesswork while the argument against third shots is purely political (the belief being that it is immoral for rich countries to be offering third shots before poor countries have had two or even one in many cases).

https://www.drugwatch.com/health/vaccine-schedule/
1377. South Korea gives final approval for Novavax. A good move and a great vaccine.
1378. The reason that so few people with boosters are getting very sick is substantially tied to the T cell response which is amazingly robust considering the vaccines were built 2 years ago against the substantially different ancestral strain.

https://www.medrxiv.org/content/10.1101/2022.01.16.22269361v1
1379. Immunity induced by vaccination followed by a breakthrough infection several months later offers better protection against Omicron than does vaccination with infection soon after. This implies that countries that saw large numbers of Delta infections in late 2021 could reasonably be expected to have some advantage against Omicron. We are not yet seeing that in the UK or the US, however.
https://www.medrxiv.org/content/10.1101/2021.12.28.21268481v1
Omicron Virus Update
1380. Early data showed that Omicron replicates 10x more slowly in the lungs but 70x faster in the bronchi. But now we see that faster replication in the bronchi, while it may shorten the time to infectiousness, is not leading to overall higher viral loads with Omicron. In fact, viral titers peak at lower levels and viral clearance is a bit faster with Omicron compared to Delta. However, the authors warn that there is substantial variation among patients and this should inform isolation recommendations to be more conservative if the goal is to break the chain of transmission. If Omicron has a lower viral titer, why is it so contagious? My note: Omicron is likely more contagious because of a combination of immune evasion, robust fomite transmission (not just airborne), and possibly better binding/faster replicating viral dynamics that may lower the minimal infectious dose and/or increase aerosol titers during speech, especially early in the course of infection when patients are more likely to be asymptomatic, especially if they are underimmunized (less than 3 shots or less than 2 shots plus a prior infection).