
COVID-19 Weekly Briefing for Monday, January 31, 2022
COVID-19 Weekly Briefing for Monday, January 31, 2022

January 31, 2022, COVID-19 Weekly Briefing in summary:
A discussion of endemicity; new information about long-covid (LC) including clues for assessing LC risk continues to point toward inflammatory autoimmunity and asthma emerges as a risk factor; vaccinated people spread C19 less (including Omicron); Pfizer is testing a new Omicron-specific vaccine; vitamin D supplementation at 1k/day is a good idea but probably won't make a big difference; a new faster spreading Omicron sub-variant called BA-2 is here; Japan fared well by masking and employing the 'Three C's"–countries that act with unity fare better than those that are divided in their pandemic approach.
Pandemic v. Endemic
1399 - 1401. This week's briefing begins with a discussion of endemicity. Journalistic media and some governments such as in the UK and Denmark have begun to refer to C19 as transitioning from a pandemic to an endemic state. What does this mean and how should it inform public health policy?
As with many things in the covid-space, the term endemic is being used by different people to mean different things. For example, when some journalists refer to C19 as endemic, what they mean is that the SARS-CoV-2 virus (Scov2) has, for all practical purposes, established itself permanently within the human population and therefore, policies aimed at eradicating it (such as nationwide lockdowns) are misguided. These are reasonable points but have little to do with whether or not C19 has become endemic.
And, when governments such as Denmark and the UK justify the lifting of all public health mitigation measures by referring to C19 as endemic, what they mean is that, from a societal perspective, the time has come to accept not only the presence of C19 but the high risk of contracting it as a normal part of everyday life, as, for example, we accept colds and flu without restricting or in any significant way changing our usual behaviors and routines. But this use of the term endemic is at least as far from the scientific meaning as the journalistic one and represents a kind of politicization of the word–an attempt to add the patina of science to decisions that are political in nature.
In Denmark, for example, the uncoupling of soaring case rates from declining death rates is most likely what is driving their government’s decision to remove virtually all covid mitigation measures. What they are really saying is that if the risk of dying is low, then, for the sake of the economy, getting C19 is acceptable. This line of reasoning, irrespective of its merit (or lack thereof), is in no way informed by the concept of endemicity.
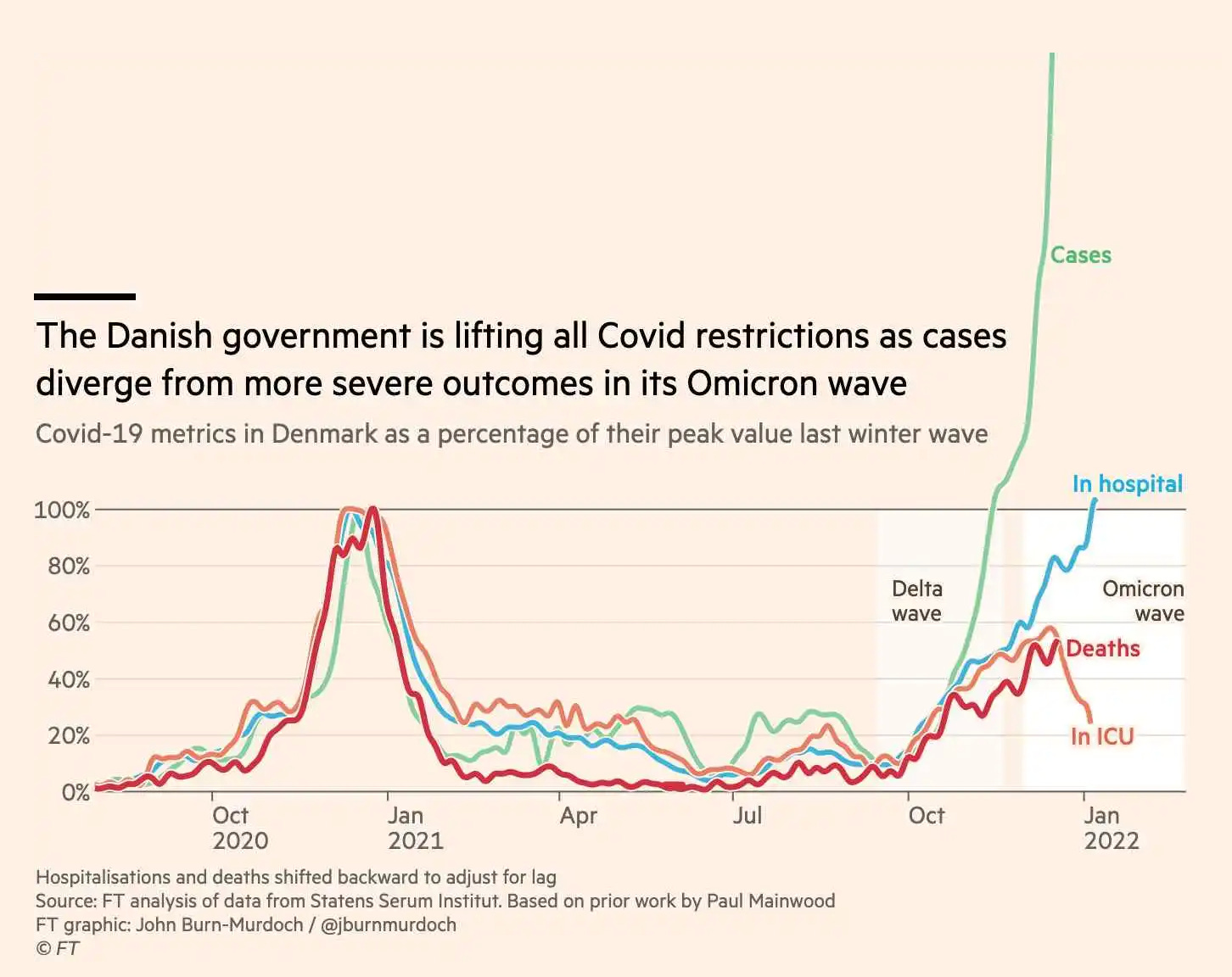
So what does the term endemic actually mean? In epidemiology, endemicity refers to the concept of a steady-state prevalence of a particular disease within a population over time. As the graph above demonstrates in stark visual terms, even if we accept that Scov2 is here to stay (we should) and even if we were to embrace a political decision to lift virtually all public health mitigation requirements including masking, quarantining, vaccinating, distancing, etc., in order to reinvigorate a flagging economy, confident that, despite high case rates, the mortality rate will be low, the prevalence of this disease is anything but stable over time.
C19 has not yet established a baseline prevalence among any population in any geographic area in the world. According to the CDC, pandemics (epidemics taking place contemporaneously in many countries) may be defined as any of the following:
A recent increase in the amount or virulence of an infectious agent,
The recent introduction of the agent into a setting where it has not been before,
An enhanced mode of transmission so that more susceptible persons are exposed,
A change in the susceptibility of the host response to the agent, and/or
Factors that increase host exposure or involve introduction through new portals of entry.
Omicron clearly meets the scientific/epidemiological definition of a pandemic. Far from being stable, it is causing waves of cases due to enhanced modes of transmission including immune evasion, and creating a new clinical presentation that includes high amounts of mucous production which enhances fomite transmission (the ability to spread through touch). C19 is, at this time, very much still pandemic, not endemic.
This is not just a question of semantics. Misuse of the term is now driving public discussion and health policy. At its core, the argument for broadly lifting public health measures is that C19 has become like a cold or flu. But these are false comparisons. Not only is C19 not stable over time but with somewhere between 10-30% of Scov2 infected people going on to develop chronic mental and physical disability, the hospitalization and death rates are, in the case of C19, not the only metrics of serious harm. Most of us give little thought to colds and flu until we catch one. But if there were such things as long-cold or long-flu driving high rates of chronic disability, we would undoubtedly take them far more seriously and this would inform public health strategy accordingly. Labeling C19 as endemic is a rhetorical device meant to distract public awareness from this reality in order to advance economic and political objectives.
And, as I have pointed out on numerous occasions, long-covid (LC) represents only one commonplace repercussion of C19 having potential long-term implications for public health, workforce productivity, the healthcare system, and the burden on society as a whole. Compelling data have accumulated showing that even among those who do not go on to develop LC, widespread organ tissue injury is common, including loss of renal function, cardiac and pleural scarring, loss of brain gray matter, endothelial injury, and diminished sperm count. If these were similarly common sequelae of colds or flu, we would treat those infections with significantly more concern.
C19 is here to stay. Public health policy aimed at the eradication of Scov2 is misguided. And keeping the economy functioning at a high level is important. But an economy staffed by workers, a growing share of whom suffer from chronic fatigue, brain fog, or cardiovascular, pulmonary, hepatic, renal, or pancreatic disease, may, in the long run, be more economically damaging than a few more months of being short-staffed. It is government’s job to create nuanced public health policy that balances all these factors. Instead, in most countries, we continue to see binary messaging that swings back and forth in wide arcs of lockdowns and ‘freedom days’, alarm and denial, pandemic and endemic.
Let’s remember what happened in the UK last summer when, at the peak of the Delta wave, PM Boris Johnson declared July 19, 2021, as 'Freedom Day' and lifted virtually all public health restrictions including masking, distancing, and vaccination requirements (a binary paradigm).
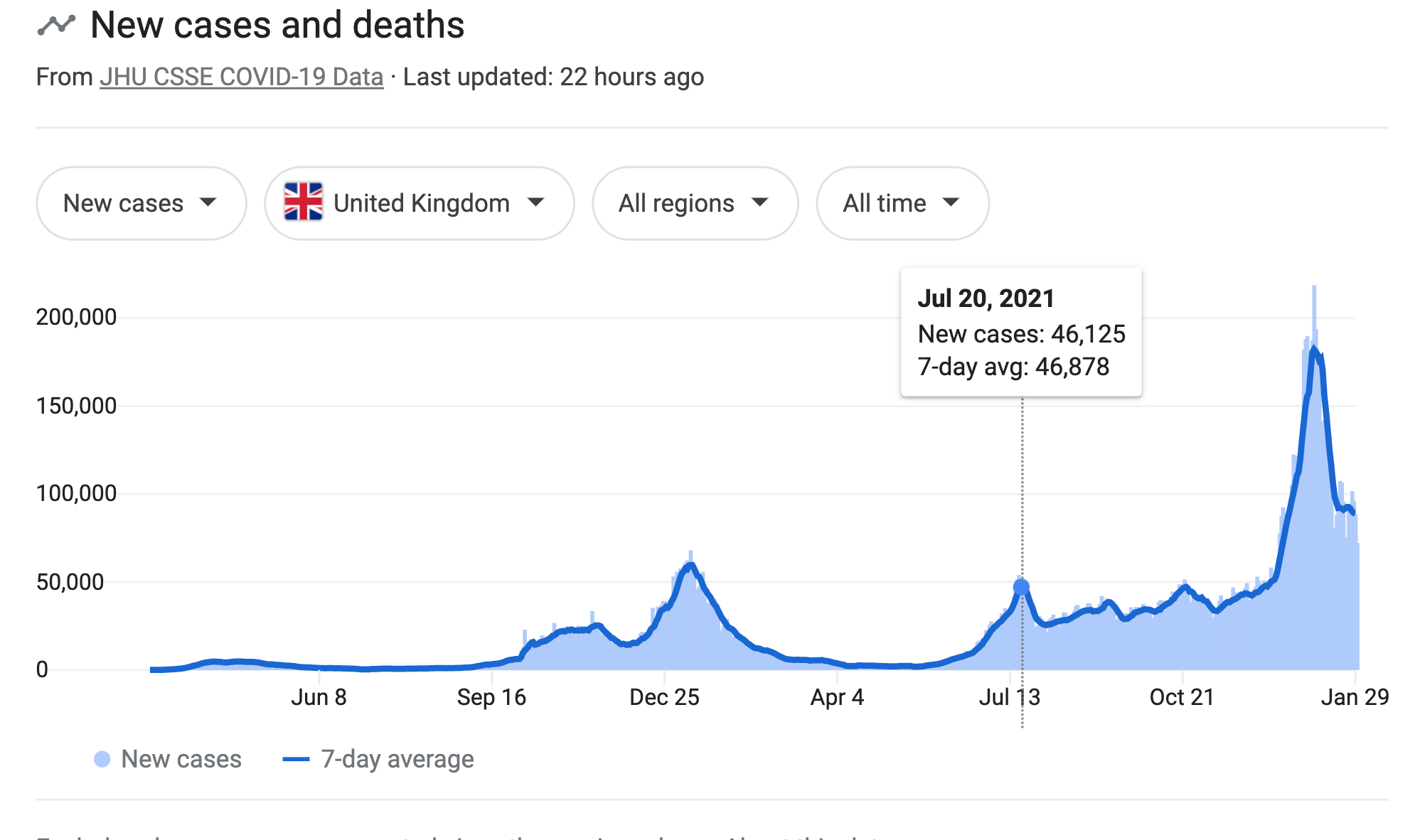
The next day, case rates began to plummet and for a short time, Johnson seemed either supremely lucky or eerily prescient. But within a few short weeks, it became evident that without reasonable public health measures, case rates would never return to low, pre-Delta levels. And there are early signs based on the above graph that a similar pattern (possibly with even higher daily case rates) is recurring now, with Omicron.
My take: We are getting close to having ubiquitous therapeutics that will tilt the game in our favor by allowing us to treat exposures and infections instantly, significantly mitigating the risks of LC, organ tissue damage, hospitalizations, and transmission. We are also close to having intranasal HCOV vaccines that will be durable and more protective than the current variant-specific ones. Allowing the disease to wash over us now, accepting infections with their risk of chronic and/or delayed-onset disease and disability is, in my opinion, a short-sighted, impulsive, and misguided strategy. We have endured 2 years of masking and behavioral restrictions. We can tough it out for a few more months if it means sparing millions of people brain fog, chronic fatigue, early-onset dementia, and a host of other outcomes that can likely be expected among those who contract C19. With new variants on the way, including those likely to have significantly enhanced immune evasion capable of causing reinfections, crookedly wrapping C19 in the concept of endemicity in order to declare the pandemic over seems a bit like taking off our collective helmet and lighting up a celebratory cigarette during the tail end of a protracted war–that is to say, understandable but unnecessarily risky, and ill-advised.
________________________________________________
1402. It has been previously shown that at 3-6 months after Scov2 infection, despite the presence of ongoing respiratory morbidity in some LC patients, proteins associated with acute inflammation expressed in plasma return to normal. This study evaluated the immune cell and protein expression (435 separate proteins were evaluated) in the airways as well as peripheral blood in a group of previously hospitalized (for C19) LC patients with persistent respiratory symptoms and pulmonary radiological abnormalities > 3 months post-discharge. The results were compared to healthy (pre-covid) controls.
Abnormal proteins associated with apoptosis, tissue repair, and epithelial injury continue to be expressed in the airways but not in the blood of LC patients with persistent respiratory symptoms. Persistently elevated LDH and albumin in the airways suggest ongoing cell death and damage to respiratory barrier integrity in LC patients with chronic pulmonary symptoms. This was not seen in any of the healthy controls. Those with more severe chronic airway disease had higher levels of killer T cells and those with more widespread lung dysfunction had increased B cell concentrations and altered monocyte subsets. These proteomic and cellular abnormalities seem to resolve over time (follow-up at one year), at least among some LC patients who have post-covid pulmonary syndromes. The findings were not linked to the severity of the acute illness.
1403. Patients who go on to develop LC showed a distinct immunoglobulin 'signature' compared to those who were infected but did not develop LC or uninfected controls. While LC and non-LC populations had similar IgA and IgG levels, the LC population had significantly lower levels of IgM during the acute infection and at 6 months follow-up. IgG3 was also lower among the LC population. The odds of developing LC were increased by the following:
Had more numerous symptoms during the acute infection.
Were sicker during the acute infection.
Had PMH of asthma.
Had higher concentrations of inflammatory markers such as CRP and TNF during the acute infection.
Striking findings: 94% of those with PMH of asthma developed PACS/LC (persistent symptoms beyond 3 weeks post-OOS) and 71% developed post-COVID-19 syndrome (PCS) defined as persistent symptoms > 12 weeks post-OOS. By contrast, 59% of those without PMH of asthma went on to PACS/LC and 42% went on to PCS. Interestingly, both healthy controls and infected patients with a history of asthma had lower serum IgG3 concentrations compared to those without a history of asthma. So something about asthma causes suppression of IgG3 which may predispose to LC/PCS. Even more striking: this same altered 'antibody signature' is also seen among patients with chronic fatigue syndrome (CFS/ME).
https://www.nature.com/articles/s41467-021-27797-1
1404. 10 out of 13 patients with LC cognitive symptoms had anomalies in their cerebrospinal fluid which were not seen in any of the participants who did not have LC cognitive symptoms. Lumbar punctures were performed approximately 10 months post-OOS. More than 3/4 of those with LC cognitive symptoms had elevated CSF protein and abnormal oligoclonal band (OCB) patterns which were consistent between them. OCBs are antibodies (typically IgG) and are seen in the CSF of patients with certain autoimmune diseases such as SLE and in 95% of patients with MS. They indicate inflammation of the central nervous system. The fact that they were found in > 75% of patients with LC and in none of the controls adds more evidence to the theory that chronic inflammation, possibly caused by the virus triggering an autoimmune process during infection, may be causally related to LC.
https://onlinelibrary.wiley.com/doi/full/10.1002/acn3.51498
1405. Vaccinated participants who had breakthrough infections were 54% less likely to report headaches, 64% less likely to report fatigue, and 68% less likely to report muscle pain compared to unvaccinated who got infected. These symptoms were similar between vaccinated and those who had not (to their knowledge) ever been infected. Note: the study ended just before Omicron.
https://www.medrxiv.org/content/10.1101/2022.01.05.22268800v2
1406. Pfizer initiates clinical trial for a new vaccine tuned to Omicron in light of reduced vaccine effectiveness (VE) against infection with the new variant. My note: New variants are likely to continue to emerge and, as we head into Phase II of the pandemic in which they will likely have significantly enhanced immune escape, updating vaccines to follow each new variant or lineage is probably not the way out of the pandemic. Rather, we will need pan-coronavirus vaccines that target the less mutation-susceptible epitopes shared by Scov2 and other human beta coronaviruses. This will create a base of immunity on top of which effective therapeutics such as Paxlovid (p.o. or, better yet, in a nasal spray form) can enable people to quickly shut infections down.
1407. A Danish study of 12K households shows that fully vax'd (3 doses) people spread Omicron less within their households compared to partially vax'd (2 doses) who in turn, spread it less than unvax'd. The overall secondary attack rate for Omicron was 31% compared to 21% for Delta. My note: We should remember that although Omicron is highly contagious (about 30% more than Delta), throughout the pandemic some people spread more than others and the household attack rate is still only about one in three among unvax'd/partially vax'd and lower still among fully vax'd. So, it is not inevitable that if someone gets it, the whole household will get it so isolation makes sense with daily RATs beginning on day 6. If RATs are negative for 2 days in a row, beginning on day 6 of isolation, an infected household member can break isolation but should still take reasonable precautions within the home, bearing in mind that Omicron likely has both airborne and fomite transmission.

https://www.medrxiv.org/content/10.1101/2021.12.27.21268278v1.full-text
1408. So-called recombinant 'Deltacron' does not exist. https://www.nature.com/articles/d41586-022-00149-9?utm_source=Nature+Briefing&utm_campaign=8ea8646386-briefing-dy-2022021&utm_medium=email&utm_term=0_c9dfd39373-8ea8646386-46403182
1409 - 1411. Maria Van Kerkhove at the WHO pronounces that the next variant of concern (VOC) "will be more transmissible than Omicron." It is likely that she is basing this on the recent discovery of BA-2, the new subvariant of Omicron (Omicron is also known as BA-1). BA-2 is estimated to be 1.5 times more transmissible than BA-1 but so far, does not appear to be more virulent or diminish vaccine effectiveness (VE) against severe disease. BA-2 is gaining market share from BA-1 in Denmark and has shown up in about half of US states. Will it take over here to cause a second huge wave?
Van Kerhove also warns against assuming new VOCs will be less virulent. That seems to like the sort of measured statement one would expect from a puplic health expert and it’s advice worth heeding–we should not assume anything. When I wrote recently that the pandemic might be moving into Phase II where we would likely see mutations favor immune escape and that that would impact both the transmissibility and virulence of the virus, I was not making a hopeful assumption (at least, not consciously). I based that, in part, on data showing that many countries are now reaching > 90% immunity combined with a fairly consistent drop over the last 2 years in the virulence of Scov2 with successive VOCs.
BA-2 might take over here as it appears to be doing in Denmark. It could drive another wave, although most public health experts don’t think it will. If it does, then Omicron (BA-1) will not have been the transitional variant to usher in Phase II of the pandemic. Perhaps that will fall to BA-2 or another variant as yet to be identified.
Or perhaps things will unfold in a completely different manner than anything I can imagine. Maria Van Kerkhove has been wrong about some big things during the pandemic. She said that asymptomatic transmission was very rare (it's common) and that there was no evidence that C19 is an airborne disease (there is a mountain of such evidence). Let's see if her latest pronouncements turn out to be prescient.
https://www.cnbc.com/2022/01/25/the-next-covid-variant-will-be-more-contagious-than-omicron-who-says.html
https://www.cnbc.com/2022/01/28/the-new-bapoint2-omicron-subvariant-is-already-circulating-in-half-of-us-states.html
https://www.ft.com/content/037a3ac9-830b-4592-9ff3-feed2008bdb7
1412. This review of vitamin D studies concludes that we don't know if it helps but 1,000 iu/day is reasonable to take. It might or might not have some benefit in preventing infections or reducing progression to severe disease but it is not harmful and many in the high-risk category for progression of C19 are also in the high-risk category for low Vit D (older people especially who tend to avoid the sun and darker-skinned people).
https://www.mdpi.com/2072-6643/14/3/464/htm
1413. Revisiting the 'Three C's": Early in the pandemic, I reported on Japan's approach to public health. They created a simple message to avoid:
Closed spaces,
Crowds, and
Close contact.
They also performed high-level surveillance. Understanding that C19 spreads stochastically with a small number of people infecting dozens or hundreds of others while most people don't spread it at all, they used backward contact tracing to find the superspreaders and stop them from continuing to infect others widely (rather than following the subsequent contacts of infected people, most of whom were not spreaders). Japanese experts also grasped, from the earliest studies, as our office did, that C19 was acting like an airborne disease, and mandated masking. How did they fare compared to the US by keeping this strategy of universal masking and the ‘Three C's’ going over the last 2 years, ramping it up during periods of higher case rates, and relaxing it a bit during lulls?
Japan: 146 deaths per million people
US: 2,590 deaths per million
https://www.nytimes.com/2022/01/24/opinion/japan-covid.html?referringSource=articleShare