

COVID-19 Weekly Briefing for Monday, January 23, 2022

COVID-19 Weekly Briefing for January 23, 2022, in summary:
Omicron update this week is courtesy of Eric Topol; RATs will probably replace PCR testing as they continue to be validated for clinical use; 3 shots of vaccine are holding up well at 4 months and will likely do so long-term against Omicron hospitalizations; Omicron is less virulent in kids; discussion of long-term effects of Scov2 infections on the brain; visceral fat isn't always reflected in BMI; A non-structural protein in RSV similar to ones in other single stranded RNA coronaviruses, like Scov2, likely plays a role in the cytokine storm; MS appears to be triggered by EBV infections (mono) which can cause neurological deficits (ME/CFS) that overlap with long-covid: an exploration of the mechanisms.
Omicron Update
1381. This week I am going to defer to the great Eric Topol who has put together what I think is the best summary of what we currently know about Omicron. In a nutshell, 3 shots of vaccine are 50+% protective against infection (which is the traditionally recognized acceptable level for approval by the FDA) and 90% protective against hospitalizations and deaths.
This widely reported divergence of outcomes with Omicron (protection against infections is significantly down but protection against developing severe disease remains amazingly high), combined with abysmal messaging from the CDC, has understandably led to an irrational loss of faith in what are truly great vaccines.
The waves caused by Omicron all over the world seem to be steeper and shorter-lasting than prior VOCs, but how far down the wave comes after it crests is not consistent and it looks like some/many countries may not see the return to very low pre-Omicron case rates (the way South Africa did) anytime soon.
Although most advanced countries have seen a dramatic uncoupling of cases and hospitalizations, not all have, and the US is particularly not glimpsing Omicron’s silver lining, with soaring hospitalization and death rates. Why? We have among the lowest primary vaccination and booster rates in the advanced world thanks to unregulated disinformation (my note).
Omicron is less intrinsically virulent but it is not just a cold and without prior immunity, the sheer number of infections is bringing us to new pandemic records of hospitalizations. We need intranasal pan-coronavirus vaccines (something I have been saying for a while and have predicted will be part of the transition from phase II to phase III of the pandemic when we regain an acceptable new normal). I hope you enjoy this 10-minute read and linger a bit on some of the graphs.

Testing Update
1382. Unfortunately, (the also great) Michael Mina has C19. Below are his rapid tests over the first 6 days of symptoms:
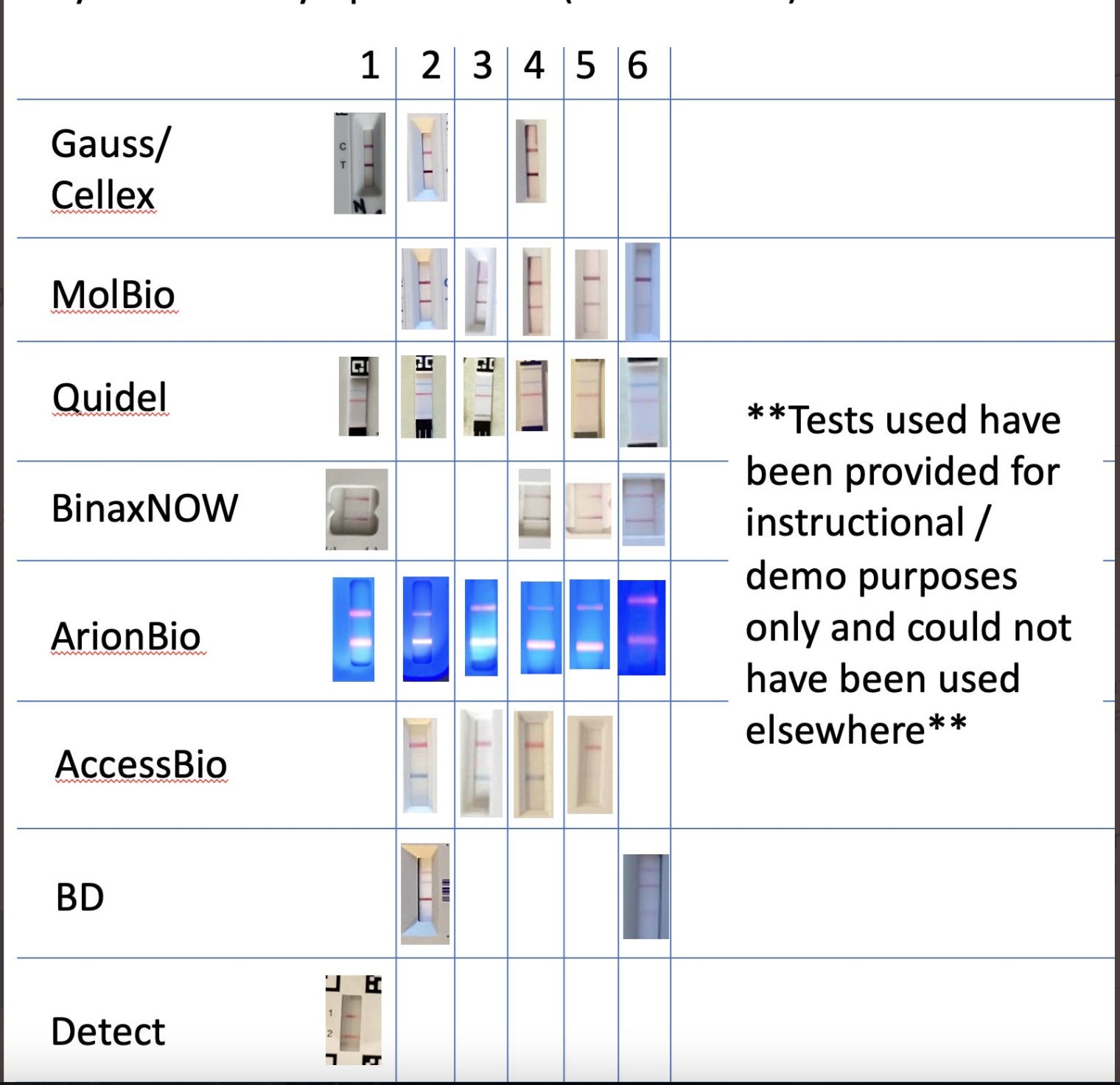
Three striking points here:
He used the standard nasal swab technique, not the (likely more accurate) throat and nose swab technique that we prefer.
Nevertheless, all 8 of the different rapid tests he is using daily are accurately registering the presence of the virus.
He continues to test positive at 6 days post-OOS!
What does this mean? For one thing, the virus colonizes the nose sooner in the course of the infection in some people than in others. It is also stunning to see how, even at 6 days post-OOS, a young, healthy, triple-vax’d person can be at/near the peak of his viral titers. Clearly, the CDC recommendation to isolate for just 5 days and then break isolation without the need of a negative test, is not based on rational public health policy. In this case, Michael Mina is still likely highly infectious 6 days post-OOS! This fact validates our understanding that among people with strong prior immunity, immunity symptoms can begin very early in the course of infection–perhaps as soon as 1-2 days post-exposure, and that the time to the peak of viral titers may be longer as immunity slows down the ascent of viral titers. Testing positive on day 6 of symptoms should not be surprising in this scenario and indeed, we are seeing this with many of our patients who are young, healthy, and triple-vax’d or double-vax’d with a prior infection.
It also shows that RATs are more reliable when used strategically (daily testing, preferably using a combined throat and nose swab, best in the middle of the day) than was initially believed. RATs are more convenient, less expensive, and provide faster results than PCR tests. In addition, RATs are better suited to adjudicate the end of quarantine/isolation. Why? PCR tests, which look for viral nucleic acids (Scov2 RNA), are extremely sensitive because they involve sequential amplification of the collected sample. Each amplification is known as a ‘cycle threshold’ (Ct) and even tiny amounts of viral nucleic acid that can remain long after infection may be detected with enough amplification. Therefore, it is not uncommon for people to continue to test positive on lab-based PCR testing for several weeks after they are no longer infectious. By contrast, RATs are only positive when viral titers are very high–at or close to their peak. So, whereas a positive PCR test does not necessarily indicate that person is infectious, a positive RAT test does and this makes RATs more useful for determining whether or not a patient can end quarantine/isolation. Here at our office, we use the rule of two negative RATs, two days in a row, beginning on day 6 of isolation, as grounds for return to work.
https://twitter.com/michaelmina_lab
1383. At first, this study is going to seem scary but stay with me... Of 1103 positive RATs followed by PCR for confirmation, from > 900K tests conducted in 537 workplaces, 42% turned out to be false positives. However, thanks to close surveillance, 60% of the false positives were found to have come from just 2 workplaces that were using RATs from the same lot-batch of Abbott's Panbio COVID-19 Ag Rapid Test. "The results demonstrate the importance of having a comprehensive data system to quickly identify potential issues." With the ability to identify batch issues within 24 hours, workers could return to work, problematic test batches could be discarded, and the public health authorities and manufacturers could be informed. False negatives with RATs are common when administered too early or late in the infection, from incorrectly performing the self-test, or (my note) from performing the test using the instructions on the box to perform just a nasal swab if it is early in the disease course before there is sufficient migration of the virus from the throat to the nose to enable detection (though this was clearly not the case for Dr. Mina). Critically, despite a bad batch of tests that led to 42% of positive results being false, the overall rate of false positives was still low (462 false positives out of 903,408 tests administered). RATs should be performed daily for several days using combined throat and nasal swabs, best in the middle of the day. Positive test results are indicative of high viral titers and that implies infectiousness.
https://jamanetwork.com/journals/jama/fullarticle/2788067
Vaccine Update
1384. 3 shots are highly protective against hospital admissions for Omicron at up to 4 months:
Up to four months following the third dose of Pfizer VE remained high (≥89%) against omicron-related hospitalization. Longer-term durability, however, remains unknown.
https://papers.ssrn.com/sol3/papers.cfm?abstract_id=4011905
1385 - 1386. However, without releasing the specific data, there is early reporting from Israel that fourth doses of Pfizer and Moderna vaccines, though they help to restore antibodies to levels seen following the third dose (or higher), are not having the clinical effect that was hoped for of preventing infections. In short, there seems to be only a small added benefit to the fourth shot among immunocompetent.
How are Kids Doing?
1385. For children under age 5, first-time C19 infections occurring when Omicron predominated (Omicron prevalence > 92%) were associated with significantly less severe outcomes than first-time infections in children under 5 when Delta predominated.
https://www.medrxiv.org/content/10.1101/2022.01.12.22269179v1
Long Covid and The Brain
Throughout the pandemic, the premier public health agencies in the US have turned a blind eye toward the bundled issue of chronic and delayed onset disease following C19 infections. In these briefings, I have provided some of the more interesting studies which represent only a small fraction of the data in support of what may be the most costly aspect of C19 in terms of overall public health and workforce productivity: the long-term disability that infection with this virus looks likely to cause in tens of millions of people–including among those who are young and suffered only mild acute illness.
We now know that Scov2 can infect virtually every organ because the cells of nearly all body tissues express ACE2. In addition to long-covid (LC), scarring in lungs and on the heart; an estimated loss, on average, of 20 years of renal function; low sperm counts; destruction of brain gray matter in the areas of smell, taste, and memory; and numerous other findings that bode for delayed-onset health consequences have been reported in the medical and scientific literature and have been included regularly in these Weekly Briefings.
It is likely that somewhere around 10-15% of infections are going on to cause LC (we have two team members with it) and we don't yet understand what the consequences of this will be on their long-term health. Countless others who have not developed LC may nevertheless be at significantly higher risk for dementia, heart arrhythmias, stroke, renal failure, sterility, asthma, emphysema, diabetes, and a host of other chronic health issues.
And yet, the CDC continues to promote public health policies that favor the endpoints of keeping the economy going and preventing hospitalizations and deaths at the exclusion of lowering the risk of infections. In my view, this may be seen in retrospect as the greatest misstep of all from the smartest, best-educated, well-intentioned public health experts in the country, who have racked up no small list of missteps during this pandemic. Here I present some new data on how C19 is affecting the brain. In a nutshell, Scov2, likely through molecular mimicry, looks like it may be provoking sustained auto-immune CNS activity that elevates inflammation in the brain.
1386. Over the course of their infections, older patients hospitalized with C19 had elevated levels of UCHL1, total tau, and phosphorylated-tau-181 (all of which measure the death of or injury to neurons in the brain). They also had elevated neurofilament light chain (which increases when nerve axons are injured), GFAP (which measures damage to glial cells), and amyloid-beta 40 and 42 (proteins that build up in Alzheimer's). 251 older patients, all in generally good health with no history of dementia or cognitive decline before their C19 infections, were split into two groups–those with and those without new-onset neurological symptoms attributed to C19. Results showed these 7 brain damage markers were > 60% increased among patients who developed neurological symptoms compared to those without neurological symptoms. Comparing both groups against uninfected controls without dementia, with mild dementia, and with Alzheimer's, C19 patients who developed neurological symptoms had the highest levels of these 7 neurological injury markers (higher even than those with Alzheimer's!).
https://alz-journals.onlinelibrary.wiley.com/doi/10.1002/alz.12556
1387. PET scans which can demonstrate neuronal injury and CNS inflammation, even in the absence of MRI findings, show pathological results in two-thirds of LC patients, demonstrating predominantly frontoparietal hypometabolism (impaired glucose uptake). This pattern was confirmed by comparison with a control sample and showed a high correlation with the Montreal Cognitive Assessment performance. There can hardly be any question that patients with LC have sustained CNS injury.
https://academic.oup.com/brain/article/144/4/1263/6209743
1388. LC presents with predominantly neurologic symptoms including impaired memory, concentration, and ability to accomplish everyday tasks, headaches, loss of smell/taste, and/or intractable fatigue that strongly resembles chronic fatigue syndrome (CFS)/myalgic encephalomyelitis (ME). Most people with LC are under 50YO, were healthy and active prior to covid infection, and were never hospitalized during their acute illness (characterized as having had mild C19). CFS/ME is commonly seen after other infections such as infectious mononucleosis and Lyme disease and is generally understood as a postinfectious syndrome.
CSF analysis among C19 patients with neurological symptoms rarely shows viral nucleic acids but routinely shows up-regulated expression of interferon-regulated genes in dendritic cells, along with activated T cells and natural killer (NK) cells. This is accompanied by an increase in interleukins not seen in blood plasma, and T cells and antibodies that recognize epitopes on the spike protein and cross-react with neural antigens. While the possibility of persistent CNS infection with limited viral replication cannot be entirely excluded (remember the recent dog-sniffing study), the preponderance of the evidence suggests that the neurological consequences of LC are the result of injury caused by infection followed by chronic inflammation caused by the initiation of autoimmune processes. There is still a plausible case to be made for vascular injury/endothelial dysregulation with thrombotic microangiopathy (microscopic blood clots) in the brain in the absence of clinically apparent stroke as having been demonstrated by MRI in some studies. But the evidence of autoimmunity is mounting…
https://www.science.org/doi/10.1126/science.abm2052
1390. Different IgG autoantibodies (AABs) were compared between four groups:
Unexposed pre-pandemic healthy subjects.
Patients hospitalized with acute moderate to severe C19.
Convalescent C19 patients who had asymptomatic or mild symptoms during the acute phase with samples obtained up to 7+ months post-infection.
Unexposed pre-pandemic subjects with SLE.
Total IgG and IgA levels were also measured from subjects in groups 1-3 to assess non-specific pan-B cell activation. AABs were higher in currently infected and convalescent as was the general expansion of the B-cell compartment, even compared to those with lupus prior to the pandemic, supporting the initiation of autoimmune responses during acute moderate, and severe C19, and after mild C19 for at least seven months.
https://www.medrxiv.org/content/10.1101/2021.01.21.21249176v1.full-text
1391. Blood samples from 177 people with prior C19 were compared against samples taken from healthy people prior to the pandemic. All those with confirmed C19 had elevated levels of autoantibodies (AABs) commonly seen in chronic inflammatory conditions like SLE and RA, directed at specific organ systems and tissues such as joints, skin, and the CNS. The overall AAB response was more robust in women following asymptomatic infections and more robust in men following symptomatic infections. Critically, the AABs observed included distinct antigens with molecular homology with Scov2, suggesting molecular mimicry as the initiating mechanism of autoimmunity.
https://translational-medicine.biomedcentral.com/articles/10.1186/s12967-021-03184-8
Note: this thread picks up again below in the 'COVID-Adjacent' section.
COVID-Adjacent
1392 - 1393. We have all been using the very convenient BMI metric for years to make diagnoses and manage patients. But while BMI can be useful when looking at extremely large populations, its value in understanding and managing individual patients is less clear. A 6' tall man who weighs 215 lbs. and has 8% body fat is considered obese by BMI. Inversely, a small-breasted and buttocked woman may be healthy by BMI standards and still have pathophysiologically significant visceral fat including non-alcoholic fatty liver disease (NAFLD).
This study demonstrates the pro-inflammatory and therefore, pro-chronic disease risks of excess visceral fat (VF) irrespective of BMI. We should consider looking beyond BMI alone when managing patients with positive family history, diabetes, hypertension, hyperlipidemia, sleep apnea, or other risk factors for 'visceral obesity' and include ultrasound imaging for those with abnormal liver panels, even if they are not overweight or obese on the BMI metric, according to the WGO.
Why is this covid-adjacent? Because the greatest mortality risk in the acute setting of C19 is the initiation of the cytokine storm which can progress to ARDS and may play a role in initiating chronic illness including possibly autoimmune problems post-infection, and patients with high VF are at higher risk for developing the cytokine storm.
https://www.biorxiv.org/content/10.1101/2022.01.19.476711v1
1394. RSV contains a protein (NS2) that stabilizes and helps prevent degradation of Beclin-1. Beclin-1 is responsible for activating autophagy which helps clear the virus from infected lung cells. But NS2 also impairs the antiautophagic homeostatic effect of ISGylation on Beclin-1. These two effects exerted by NS2 together can create a glut of active Beclin-1 and drive excessive inflammatory autophagy (of lung cells) that can lead to pneumonia/ARDS. Does this process sound familiar?
In the US, RSV causes 160,000 deaths a year, primarily among infants, the elderly, and immunocompromised. This could have ramifications for therapeutics not only against RSV but other single-stranded positive-sense RNA viruses that encode nonstructural proteins, including influenza and Scov2. These nonstructural proteins are not packaged in the virus particle, they are expressed in infected cells and act to antagonize the innate immune response. Therapies that target non-structural proteins such as NS2 (or, in the case of Scov2, NS1) could potentially tamp down the kind of viral immune-dysregulation that can lead to ARDS.
https://journals.asm.org/doi/10.1128/mbio.03528-211395.
For example, 50% of hospitalized patients with C19 had autoantibodies (compared to 15% of controls) and showed higher levels of antibodies against Scov2 Nonstructural Protein 1 (NSP1) and Methyltransferase (ME). The authors conclude that Scov2 causes the development of new-onset IgG autoantibodies in a significant proportion of hospitalized C19 patients and is positively correlated with immune responses to Scov2 proteins.
https://www.medrxiv.org/content/10.1101/2021.01.27.21250559v1
1396 - 1398. Only one out of 801 multiple sclerosis (MS) patients was seronegative for Epstein Barr virus (EBV) at the time of MS onset. This offers compelling data implicating EBV as a trigger for the development of MS. How does it work? There are many proposed mechanisms but the preponderance of evidence tilts toward molecular mimicry leading to autoimmunity with studies showing that serum antibodies from MS patients to the EBV protein BFRF3 cross-react with the cytoplasmic protein septin-9 which is upregulated following traumatic brain injury and associated with neuronal demyelination. MS patients are also cross-reactive between a sequence of amino acids on the viral protein EBVNA-1 and myelin basic protein (MBP) believed to be necessary for maintaining the correct structure of myelin by helping regulate lipids in the myelin membrane. Antibodies in the CSF of MS patients that target EBNA-1 also cross-react with the CNS cell adhesion molecule, glialCAM. In fact, three contiguous regions of mimicry have been reported in a small region of the EBNA-1 protein. In short, epitopes of the virus have sufficient overlap with epitopes in the proteins of several CNS cells causing an inflammatory attack against not just the virus but the myelin sheath, axons, and ultimately, the neurons themselves.
In addition, the B cells of patients with MS can be infected by EBV and their activated progeny (plasmablasts) express a protein with adhesive properties that allow these antibody-producing cells to move from the bone marrow to the peripheral circulation and then across the blood-brain barrier (BBB), where they take residence inside the brain and meninges. The antibodies these plasma cells ultimately produce target myelin-producing glial cells initiating the pathophysiology of MS.
Why is this covid-adjacent? As we continue to learn more about the widespread organ tissue damage, including in the CNS, caused by Scov2 infections, prior investigations of viral pathogens known to cause prolonged CNS illness having clinical overlap with long-covid (a high percentage of patients with mono progress to CFS/ME) can help shed light on what we might expect down the road for the tens of millions of people who contracted C19.
https://www.science.org/doi/10.1126/science.abm7930#f1
A Data Point Worthy of Reflection
1398. A sobering moment to consider the C19 death toll. Projections based on excess mortality suggest that the official 5.5M reported deaths are only about 1/4 or 1/5 the true count.
