
COVID-19 Weekly Briefing for Monday, April 11, 2022
COVID-19 Weekly Briefing for Monday, April 11, 2022
Cell phones and brain cancer; 'dopamine fasting' for addiction; stress drives hypertension in men; black people are more susceptible to kidney injury from C19; and much more.

First, apologies for getting the Weekly Briefing out a day late. It has been a very busy week at the practice and I took the weekend off to engage in hormetic (and other) recuperative practices. Balance is the essence of good health.
Some preliminary good news about mobile phones and cancers
Mobile phones emit radiofrequency waves which, when the phone is held close to the head, are capable of penetrating several centimeters into the brain. For some time now, I have worried that mobile phone users may be at increased risk of developing brain tumors.
In fact, the International Agency for Research on Cancer (IARC) has classified radiofrequency radiation (RFR) as potentially carcinogenic, and anecdotal reports from physician colleagues over the years who have noted escalating rates of breast, ovarian, and testicular cancers among young patients who carry their cell phones in their pockets or tucked under their bra-strap led me to seek out and offer to my patients RFR blocking devices that can be easily placed under a cell phone’s shell to block the radiation ‘plume.’
Unfortunately, most of the studies that have investigated the potential dangers of RFR have been retrospective studies in which individuals report cell phone use after a diagnosis of cancer. Such studies rely on (notoriously faulty distant) memory and are often conducted on a biased population (those who have developed cancer already).
But a new, prospective study (participants were enrolled before they developed cancer) from Oxford Population Health and IARC, using data from the UK Million Women Study (an ongoing study that includes 25% of all women in the UK born between 1935 and 1950), compared about three-quarters of a million women who were surveyed about their cell phone usage, first in 2001, then again in 2011, and then followed for an average of 14 years via their electronic medical records, and showed there to be no significant difference in the risk of developing a brain tumor between those who never used a cell phone and those who used them regularly–including tumors in the parts of the brain near the ear that were most exposed to RFR.
Specifically, there was no increase in the risk of developing tumors among those who spoke on their cell phones daily, spoke for at least 20 minutes a week, and/or had done so for more than 10 years compared to those who did not use cell phones. Compellingly, the incidence of left-sided tumors among cell phone users, as with non-users, was about the same as right-sided tumors, despite the fact that most people hold the phone to the right ear far more than the left.
However, only 18% of the women in this study reported talking on their cell phones for 30 minutes or more each week so it is hard to know if these hopeful data can be extrapolated to those who talk more on their phones. My take: I think it is still a good idea to use a hands-free approach whenever possible while talking on the phone, try not to carry the phone against the body for long periods of time, and, until more data demonstrate the safety of prolonged exposure to RFR, I’m keeping my blocker on my phone.
Dopamine and addiction
In the March 28, 2022 Weekly Briefing, I discussed how pleasure and happiness are marketed to us as interchangeable concepts but are, in fact, very different from one another–both experientially and neurochemically. I made the point that chronic pleasure-seeking not only does not lead toward happiness but lures us in the opposite direction by driving excessive production of dopamine (the hormone of desire and gratification) at the expense of healthy levels of serotonin (the hormone of happiness and contentment).
Today, I would like to expand on this idea and discuss how a culture that trains us to seek pleasurable stimulation to excess, forcing dopamine production into overdrive, is at the heart of epidemic levels of addiction in the US.
What is addiction?
According to the DSM-5 (the manual used by psychologists and psychiatrists to diagnose mental illness), addictions include a variety of symptoms and behaviors that work against our ability to be happy. Two or three symptoms indicate a mild substance use disorder (SUD); four or five symptoms indicate a moderate SUD; and six or more symptoms indicate a severe SUD–also known as an addiction.
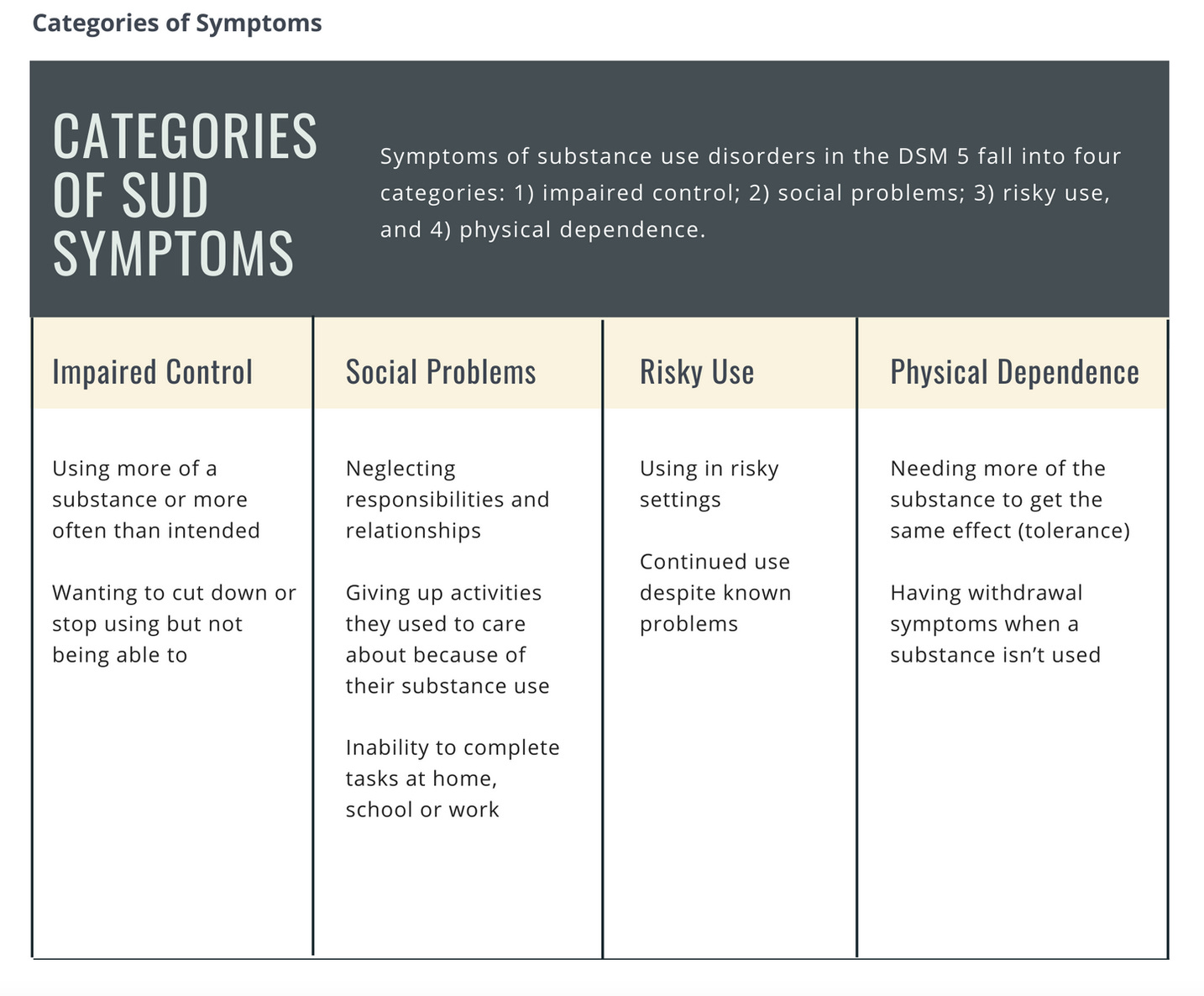
But most experts now believe that anything capable of strongly stimulating us to drive dopamine can be addictive and, on that basis, a simpler way of understanding the problem is that whenever a pleasure starts to become an obligation, when wanting becomes needing, it can be considered an addiction.
In the 3/28/22 Weekly Briefing, I discussed how stress and pleasure-seeking both drive excessive dopamine production which accumulates in a part of the brain called the nucleus accumbens (NA). When dopamine levels in the NA reach a critical threshold, the NA takes over our decision-making apparatus (the part of our brain called the pre-frontal cortex), ordering us to seek some prescriptive pleasurable stimulation. If you’ve ever found yourself making the decision to binge eat cookies late at night after a day of consciously striving to eat healthily and lose weight, that’s the NA discharging its dopamine!
After we ‘score’ (light up the cigarette, sip the cocktail, eat the cookies, etc.) our brains release euphoric pleasure hormones called endogenous opioid peptides (EOPs) which make us feel great, soothing unpleasant emotions like anxiety or loneliness that we might be chronically trying to avoid by keeping busy.
But the relief of indulgence is short-lasting. And the short-lasting nature of pleasure, along with its dependence on some external stimulation, are two of the chief characteristics that distinguish pleasure from happiness (the enduring, self-regenerating state of feeling content with oneself and one’s life).
And there is an additional, third characteristic that separates the experience of pleasure from that of being happy. Pleasure, when consumed habitually, is by its nature addictive. And addictions–obligations–constrain our freedom limiting our ability to feel happy.
The seesaw
It turns out that the neurochemical pathway by which we experience pleasure is like a seesaw. When we drive a burst of dopamine, tilting our consciousness toward pleasure, our brains push back the other way soon after, dropping dopamine levels and causing us to experience discomfort.
As described at length by Anna Lembke, MD, in her illuminating book, Dopamine Nation (Finding Balance in the Age of Indulcgence), our bodies strive to keep all hormones–including brain hormones–in a state of balance referred to as homeostasis. If we drive dopamine levels above homeostatic levels, our brain reacts to this by driving them back down.
Using the seesaw analogy, Dr. Lembke describes how pleasure and pain are experienced in the same part of the brain; the process of dopamine pushing down on one end of the plank (pleasure) is followed by what she refers to as “little gremlins” that push down at the other end (pain) to restore the seesaw to the neutral (homeostatic) position.
Critically, if we drive excessive amounts of dopamine chronically, our brains react by making more of those gremlins and making them stick around for longer periods of time afterward, tilting the seesaw not just back to homeostasis but past that, in the opposite direction of pleasure, and holding us in the experience of regret and discomfort.
How do you feel the morning after ruining a day’s good efforts to lose weight and get healthy by binging on a box of cookies late at night? If like me, you feel disgusted, regretful, and motivated by a new renewed sense of urgency driven by self-loathing to be more disciplined, then you know what those gremlims feel like.
How do you feel the morning after a night of heavy drinking or using any drug? The fatigue, headache, and general dysphoria of a ‘hangover’ are the price we pay for tilting the seesaw too forcefully into pleasure the night before.
Even ‘soft addictions’ (more about this later) like the one I have currently to coffee, act against our fullest sense of happiness. For one thing, my coffee addiction constrains my freedom a little bit. If for any reason I can’t have my morning coffee, I experience significant discomfort–physically and emotionally. My mind is not as sharp as I want it to be. I feel grumpy and if I go long enough without a fix, I will begin to go into withdrawal, including headache and extreme irritability.
I go through this about once each year, typically when I’m up to needing three cups a day to get me feeling good. I weather the withdrawal period (typically a weekend of pain and discomfort), then take a month off of caffeine during which time, as those gremlins gradually jump off the discomfort side of the seesaw, I slowly regain my natural state of good energy and mental clarity.
At this point, I can reintroduce enjoying a cup of coffee when I want it without feeling addicted. But, typically after a few months, my frequency and level of use start to climb again. By the end of the year, I’m back to where I started, addicted to coffee.
Why does this happen? The more regularly I consume caffeine, the longer the gremlins that drive dopamine down on the discomfort side of the seesaw stick around, necessitating that I drink more coffee to drive more dopamine to tilt things back toward pleasure and get the desired level of stimulation.
In addition, excessively driving dopamine over a prolonged period of time causes the brain to reabsorb some of its dopamine receptors (proteins on the surfaces of brain cells that are activated when they come into contact with dopamine).
More gremlins and fewer receptors are the body’s way of attempting to restore normal dopamine levels (homeostasis) in the context of habitual pleasure-seeking. But this is also the blueprint for addiction. The more we use, the more we need in order to get the desired effect. And the more we need, the more we use. Eventually, we are unable to produce enough dopamine to get much enjoyment from our addiction. But we keep using anyway to avoid the discomfort of going through withdrawal.
This, in a nutshell, is addiction. And it can happen with hyper-palatable foods, ‘likes’ on social media, taking risks (gambling, extreme sports, etc.), or consuming any number of chemical substances. I refer to things that cause a big enough burst of dopamine to get us hooked but not enough to take over our lives completely (like coffee) as ‘soft addictions’ and those that drive a massive dopamine release that quickly has us organizing our lives around scoring (like cocaine) as ‘hard addictions.’
Dopamine fasting
Chronically engaging in behaviors or consuming substances that drive excessive amounts of dopamine can lead to a state of dopamine deficit in which we feel depressed, anxious, and uncomfortable. Substances that are super-drivers of dopamine do this quickly but accumulating enough ‘soft addictions’ can have the same effect. Ultimately, a prolonged dopamine deficit can lead to the inability to experience joy in normal activities, lowering our ‘happiness quotient’ considerably.
When enough sticky gremlins accumulate on the discomfort side of the seesaw, life loses its color. Medicines that act to raise serotonin can sometimes help–for a while. But what Dr. Lembke recommends–and the strategy that I prefer in my practice–is what she refers to as a dopamine fast.
Similar to the process I go through about once each year with coffee, identifying and then completely discontinuing the dopamine-driving behavior(s) at first puts us into a state of deep discomfort (withdrawal). In that state, the voice inside our heads will try to convince us that all we need to feel happy again is to score the substance or engage in the behavior we’ve sworn off. And that’s half true. Scoring will put an end to the discomfort of withdrawal but once we are in a state of addiction, scoring does not tilt the seesaw enough to generate significant pleasure, and prolonging an addiction certainly does not lead to happiness.
Sticking with the dopamine fast, conscious of the fact that the pain of withdrawal is proof of our addiction and secure in knowing that it is only for a short while, eventually leads to the gremlins abandoning the discomfort end of the seesaw. As this happens and the plank gradually comes back finally to level (homeostasis), the addiction lifts, and normal feelings of health and well-being return.
New dopamine receptors pop up on the surfaces of our brain cells. We begin to drive normal amounts of dopamine from a good conversation, a walk in the woods, or a hug from a person we feel close to. As dopamine levels return to normal, we regain our sense of motivation and happiness.
How long does a dopamine fast take to do its job? It depends on whether the problem is a soft or hard addiction, how long it has gone on, the particular biochemistry of the person, and the goal. I find 30 days to be enough to reset my relationship with coffee, which typically turns toxic when I need three cups in the morning to get the feeling of pleasure and alertness that I want.
If I don’t quit at that point, I know by experience that within another month or so, even three cups will not be enough to give me the feeling that I want. In fact, no amount will. By the time I need three cups, too many sticky gremlins have accumulated and it’s time for me to start my dopamine fast. The goal, for me, is to be off coffee long enough to be able to use again in a responsible way, driven by want and enjoyment, not by need or to offset discomfort or a lack of mental alertness.
There is, of course, much more to dopamine and addiction–a subject I will return to again in future briefings.
Hypertension and emotion
Hypertension (high blood pressure) is a disease that causes more than half a million deaths each year in the US. However, in the majority of cases, there is no clear medical explanation for why some people get hypertension. Referred to as ‘essential hypertension,’ there has been plenty of speculation as to why it is common among those who seem otherwise healthy.
In this new study, hypertensive men were more likely to identify the emotion of anger in the facial images of people experiencing mixed emotions compared to men who did not have hypertension. In addition, prospectively, men who both felt angry (‘trait anger’) and overrated displayed anger in facial images were more likely to have their blood pressure go up over time.
Many clinicians would intuitively say that feeling chronically angry (and perhaps also being hyperaware of others’ angriness) are not good for one’s blood pressure. Since hypertension plays an important role in cardiovascular disease (CVD), this study, the first to show a scientific link between the emotion of anger and high blood pressure, is worthy of interest.
Diet sodas and weight loss
For years, I have counseled my patients against the use of low-calorie and/or no-calorie sweetened beverages (LNCSBs) as substitutes for sugar-sweetened beverages (SSBs) even in the context of attempted weight loss and/or lifestyle modification to improve diabetes. Instead, I have advocated for unsweetened beverages (high-quality water is best).
Why? For one thing, many/most LNCSBs contain preservatives and other additives that are likely to be or have been shown to be unhealthy. For another thing, intensely sweet drinks cause us to release dopamine and can be addicting. Some have even theorized that insulin may be released upon the sensation of sweetness even in the absence of sugar, and chronically stimulating the release of insulin blocks fat burning and causes our tissues to lose their sensitivity to the hormone’s action (which drives Type II diabetes).
However, in this systematic review and meta-analysis of 17 randomized clinical trials, LNCSBs as a substitute for SSBs were associated with reduced body weight, body mass index, body fat percentage, and fatty liver, providing benefits that were similar to those of water. At least in the short or medium term, LNCSBs could be a reasonable alternative to water as a replacement strategy for sugary drinks in overweight and obese adults at risk for (or with) diabetes who have difficulty tolerating drinking lots of water. Sometimes it’s good to be wrong.
COVID-19 Updates
Antibody tests are unreliable in kids
Blood tests are now available to tell whether or not someone has had C19 in the past. Both vaccines and infections produce antibodies, but vaccines only induce the production of antibodies against the virus’ spike (S) protein while infections induce antibodies against both the S protein and the nucleocapsid (N) protein.
The presence of antibodies in the blood after vaccination or infection is called seroconversion. In this cohort study of 57 children and 51 adults, the proportion of children with seroconversion to SARS-CoV-2 (Scov2) N-protein was half that found in adults despite having similar viral loads. This study suggests that blood tests for anti-N-protein antibodies are not a reliable way of ascertaining prior Scov2 infection in children.
One rapid test is unreliable but two are very good
As PCR tests for C19 are no longer free and much less available, more people are not testing themselves or are using home tests called rapid antigen tests (RATs). We have promoted the use of RATs at our office for some time–both as a way of testing for Scov2 infections and also as a way of determining whether or not to remain in isolation after an infection.
Our protocol is to quarantine immediately and begin using RATs 3 days after the onset of symptoms for those who are unvaccinated or under-immunized or 5 days after the onset of symptoms for those who are up-to-date (three shots plus a past infection prior to December 2021; two shots plus an infection during or after December 2021; or four shots with or without an infection).
If three consecutive RATs are negative, it is highly unlikely that the cause of the symptoms is C19. If there is a positive test, isolation is critical to avoid spreading the disease to others. Isolation can be ended the day after two consecutive days of negative RATs.
Our protocols have seemed overly conservative to many and are not the protocols being promoted by the CDC. But there has always been some question about the accuracy of RATs and our protocols take that into consideration, viewing the inconvenience of an extra day or two of testing and quarantine/isolation as a minor discomfort compared to the potential catastrophe of spreading C19.
Now, in a new high powered study, we see that while a single RAT is often inaccurate, providing high rates of false postitives (only 38% of first positive RATs were confirmed to be positive by PCR) two RATs performed on consecutive days was 94% accurate (as confirmed by PCR). Somtimes it is good to be right.
Evusheld is effective against Omicron and BA.2 according to two new in-vivo studies.
Evusheld, the long-acting monoclonal antibody cocktail made by AstraZeneca was given emergency use authorization (EUA) by the FDA for adults and adolescents (12 years of age and older who weigh at least 88 pounds) for preexposure prophylaxis for the prevention of C19 (not for treatment of infections).
It is meant for patients with moderate to severe immune compromise due to a medical condition or those taking immunosuppressive medicines or treatments who may not mount an adequate immune response to vaccination or those who have had severe allergic reactions in the past to any of the components of the currently approved vaccines.
The two antibodies contained in Evusheld (tixagevimab and cilgavimab) are coadministered via two separate injections into the arm. Evusheld may offer protection for several months.
I have not reported on this in prior briefings because it was given EUA around the time of Omicron and there were not any data until recently showing whether or not it was effective against the new variants. Now, two new studies show that Evusheld protects against both Omicron and BA.2–the variants currently in circulation.
The only problem: very hard to find. If you think you might be eligible for Evusheld and would like to speak with a physician about it, please call the office and schedule a telemedicine visit with Dr. Ehrlich: 858.450.5900
Long-covid/OTI update
We know that organ tissue injury is common after C19 and significant reductions in renal (kidney) function among those who have been infected has been well described. In a new study, we see that persons of African descent who carry two genetic variations for blood lipids (APOL1) have double the risk for acute kidney injury and death from C19 infection. Since about 13% of black people carry this genetic variation, the impact of C19 on Americans of African descent is particularly severe, even among those whose renal function was normal prior to infection.