

COVID-19 Weekly Briefing for Monday, March 28, 2022
Pleasure v. happiness; second booster shots; Florida is now openly anti-vaccination (at least for kids); and mild COVID-19 causes diabetes one year down the road.

I. Dopamine and Serotonin; Pleasure v. Happiness
The cultural construct
When asked what we most want from life, many of us would answer by saying that we would like to be happy. The pursuit of happiness is a central concept of free societies. It is enshrined as an inalienable right in our Constitution. But what does it mean, exactly, to be happy? Is it a medical concern? Should it be?
This week’s Briefing begins with a discussion of ‘cultural biology’ as it relates to our health and pursuit of happiness.
Merriam Webster’s Dictionary defines happiness as:
“a state of well-being and contentment,” but also as “a pleasurable or satisfying experience.”
In other words, according to the modern dictionary definition, happiness and pleasure are interchangeable exeperiences. In fact, this is a message we are bombarded with, explicitly or implicitly every day–whenever we linger on the manufactured Instagram post of someone broadcasting their ‘peak experience,’ watch an episode of reality television shot in the mansion of someone rich and famous, or are exposed to virtually any form of advertisement.
While you’re at Disneyland, the happiest place on earth, be sure to stop at the concession stand and have a Coke and a smile and then grab a Snicker’s bar to go because Snicker’s really satisfies.
It goes something like this: amidst the chaos of modern life, there’s an emptiness inside of you–a place where joy has gone missing. It’s not your fault. The world is a stressful place in which to live. But don’t worry, we’ve got you covered: just fill the void with (insert product, service, or experience here).
Success in modern society means having access to some of the rarest and most intense pleasure experiences ever imagined. But what effect does it have on us to live lives in which we aspire to gratification and excitement? When we have an abundance of such things and yet still feel like something is missing from our lives, does this mean we need even more?
Is having instant access to pleasure on demand what it means to be happy?
With just a few clicks, we can have our favorite foods prepared and delivered to our doorstep within the hour. We can do the same with feel-good drugs that are now legal in most states. Within a day, Amazon can ship us nearly any commodity our hearts desire. And for comparatively little money, we can fill our grocery carts with calorie and carbohydrate-dense foods scientifically calibrated with just the right combination of sugar and salt and fat to excite the pleasure centers of our brains in a way that no human ever experienced during our 200 million years of evolutionary history.
In many ways, even average citizens of advanced nations today have access to more luxury and pleasure than the kings and emperors of times past. And in many ways, our lives are also easier than they have ever been. More people than ever now work from home and meet via teleconference, eliminating the time and toil of commuting. We can do our banking, get our education, and even date online without having to shave or get dressed.
The makers and purveyors of consumer products and services are promoting the narrative that all this readily available ease and pleasure are making our lives better and that better living means more happiness. But are we more happy now than we were, say, a decade or two ago?
According to Mental Health America, the rate of suicidal ideation among US adults has increased every year since 2011. A growing percentage of children and teens have major depression with 15% having had an episode in the past year. Anxiety increased by 40% in 2018 among adults. In the six months between August 2020 - February 2021, adults with symptoms of anxiety and/or depression increased from 36% to 42%. And the rates of substance abuse have been gradually increasing across all ages for more than a decade.
These problems were exacerbated by COVID-19 (C19) but they did not start during the pandemic; they have been steadily on the rise, right alongside the progressive ramping up of access to ease and pleasure on demand.
The biology of pleasure and happiness
It turns out that happiness is not something that can be found in what we eat or drink or wear or do or own or post because, although these things promote pleasure, pleasure and happiness are not the same thing.
How are they different? In a nutshell, pleasure is a fleeting experience and is dependent upon some kind of external stimulation, while happiness is an enduring state of well-being–an experience that is self-regenerating and independent of external stimulation.
We can distract ourselves from feeling empty, bored, or anxious with pleasure. But that doesn’t heal the emptiness or fear or anxiety or boredome or absence of meaning or low self-esteem or sense of hopelessness or whatever is at the cause of our individual and collective discontent. In short, pleasure cannot make us happy and, in fact, too much pleasure might be driving a lot of our unhappiness.
The more we reach for a particular pleasure, the more diminished our experience of gratification becomes. This is known in physiology as the tolerance principle. Tolerance leads us to ramp up the dose and frequency of our pleasure-seeking which is the beginning of what I refer to as soft addiction. And addictions (hard or soft) are the enemies of happiness (more about this in a future Weekly Briefing when I will discuss tolerance, addiction, and the pleasure/pain seesaw as described by Anna Lembke, the author of Dopamine Nation; Finding Balance in the Age of Indulgence).
It may not be news to you that pleasure and happiness are different things. They feel different, don’t they? That lift from the first draw off a cigarette versus the feeling you get from working hard for a cause that you truly believe in; the short-lived buzz of a cocktail versus the enduring contentment of knowing that your child is well-situated in her life; the rush of heading out for a first date versus the coziness of going home to the person you truly love.
Excitement feels different from contentment because, as neuroscientists have been able to demonstrate, pleasure and happiness are biochemically different–the result of different neurohormonal pathways in the brain. The pleasure pathway converts an amino acid called tyrosine into dopamine, the so-called pleasure hormone, while the happiness pathway converts a different amino acid called tryptophan into serotonin, the so-called happiness hormone.
Now, although dopamine and serotonin are made in the brain, the amino acids they are derived from are not. Tyrosine and tryptophan have to be brought into the brain across a tightly controlled checkpoint called the blood-brain barrier (BBB) by a special transport protein. Critically, tryptophan and tyrosine use the same transport protein for this, called LAT1.
But there is a limited supply of LAT1 available to carry amino acids across the BBB. So, if our habits and behaviors tilt toward excessively driving the pleasure/excitement pathway, most of the available LAT 1 gets used up carrying tyrosine into the brain to make dopamine at the exclusion of carrying tryptophan into the brain to make serotonin. And if that goes on for long enough, the serotonin levels in our brains start to drop, making us feel anxious and depressed.
According to many of the world’s leading neuroscientists, the chief driver of epidemic anxiety and depression in this country is that our brains have been hacked by a culture that drives us away from each other, promotes chronic stress, and then offers compulsive pleasure-seeking as the antidote, firing the excitation/pleasure dopamine pathway to the exclusion of the happiness/contentment serotonin pathway. Once our need for excitement and pleasure begins to cause us to view contentment and real happiness as a threat to our pleasure-seeking modus operandi, we are in addiction.
Even if that addiction is to something relatively harmless, like snacking in front of the television at night, the effect, like disinformation in a democracy, is the slow erosion of the thing we most cherish–our happiness.
Marketing is a science, not an art
The people who get paid to sell us stuff are well-versed in the biology of soft addiction. They know that it’s the desire/pleasure pathway, not the happiness/contentment one that fuels sales and likes and follows.
They start by putting us in touch with the place inside of us where joy has gone missing. Even the seemingly benign image of a group of friends all smiling and enjoying a pizza while watching the game reminds us, as we sit on our sofa, clicker in hand, that others are having peak fun out there. Discontent stimulates the release of a stress hormone called cortisol, and one of the effects of cortisol is that it gins up the production of dopamine to create the feeling of want.
And it isn’t just stress that drives up dopamine. Anticipating some desired reward drives it too. When we watch that television commercial featuring a group of smiling friends lifting gooey slices from a pizza box, we experience a hit of dopamine. Bakeries often pump their exhaust out onto the sidewalk where passersby can catch a whiff of fresh-baked cookies. A few seconds later, we might find ourselves stopping in–against the diet we have been holding to with effort all day, despite the fact that stopping for a cookie might make us run late. The ping of the phone alerting us to another ‘like’ provides a small hit of dopamine too and leads us to develop a continuous vigilance over our phone…
Within the brain, dopamine builds up in a place called the nucleus accumbens (NA). The NA has the role of ordering our minds to take some pleasure-seeking action. When enough dopamine accumulates to cross a certain threshold, this activates the NA which then, for a moment, takes over our thinking aparatus.
If you have ever found yourself raiding the snack drawer late at night after a day of being mindful of your diet, you know what I mean when I say that, once the NA turns on, you are no longer the one making decisions for yourself. We are all familiar with the story of the alcoholic, three years sober, pulling into the bar on his way home from work one day for no apparent reason and relapsing into a bender. That’s the NA at work.
We’ve all been there in one way or another. The next day we feel wake baffled and disgusted. Why did we do that?–we wonder. The answer is that we were not the ones who chose to ‘break bad.’ We were rendered passive to the self-destructive pleasure-seeking experience orchestrated by the NA which had accumulated, likely because of stress, enough dopamine over the course of the day to reach the discharge threshold.
Without an understanding of this neurobiology, we are unable to make sense of our own behaviors and are left with self-recriminating inner talk about weakness, and failure. Familiar feelings of regret and shame set in, driving cortisol which in turn, drives dopamine and the cycle repeats.
In the last Weekly Briefing, I discussed the new science of metabolism and weight loss, making the case that the difficulty many of us face when trying to get to our healthiest weight is in part a function of misunderstanding how weight loss works. But there is another barrier to weight loss and that is how dopamine empowers the NA to flip a switch in our brains turning us into mindless pleasure-seekers.
So, dopamine is bad and serotonin is good? No! Like all things, it’s about balance.
This is not to frame dopamine as ‘bad’ and serotonin as ‘good’ in some epic hormonal battle. In fact, dopamine and serotonin are both essential to human happiness. Like all things, there is a sweet spot for hormones wherein too little leads to deficiency but too much becomes toxic. We need enough serotonin to experience happiness but we also need enough dopamine to keep us feeling motivated, to have something to look forward to, and to want to do the work we must do in order to achieve our goals.
In a future Weekly Briefing, I will discuss in more detail how excessive dopamine drive is causing epidemic levels of addiction. For now, let me just point out that while you may or may not have already known that excessive production of cortisol caused by stress can drive dopamine levels too high or that excessive dopamine production leads to addiction or that tyrosine competes with tryptophan for LAT1, most of us, by a certain age, have probably worked out that compulsive pleasure-seeking is not the same things as or the road to happiness.
You know the moment I’m talking about when you realize that you need something that you used to just want. How the satisfaction you once had after a bag of chips or a cocktail now barely takes the edge off–but you feel utterly compelled to have it anyway. How gratifying these urges has somehow become overly important and, simultaneously, exhausting and shaming–the opposite of a self-regenerative feeling of well-being.
As medical providers, we are focused on helping patients achieve good health. But the concept of health as the absence of an active medical diagnosis is no longer an adequate construct. Modern science is showing us that mental health and physical health are deeply intertwined. That health and happiness are two sides of the same coin. For me, being a ‘holistic’ provider is not about offering magic potions or other non-evidence-based interventions; it means viewing people comprehensively in the context of their lives, practicing with an understanding that happiness is the product of good physical and emotional health and that promoting both is the ultimate goal of every doctor-patient relationship.
II. Should we be giving/taking fourth shots of C19 vaccine?
As we know, vaccine effectiveness (VE) against infections with SARS-CoV-2 (Scov2), the virus that causes COVID-19 (C19), has waned a little with each new highly mutated variant of concern (VOC). With Omicron and BA.2, the level of protection after primary (2 shots) vaccination against symptomatic infection is now minimal.
We also know that protection against symptomatic infections (PASI) improves substantially following a third (booster) shot of mRNA vaccine–even against Omicron, as a new study from the UK, published in the New England Journal of Medicine, confirms.
Among those who received 2 shots of AstraZeneca’s vaccine, PASI with Omicron increased from 0% to 62% after a Pfizer booster (and 70% after Moderna booster) at 2 to 4 weeks and then waned to about 40% protection at about 3 months. Among those who received 2 shots of the Pfizer vaccine, PASI with Omicron increased from 8% to 67% at 2 to 4 weeks after a Pfizer booster (and 74% after Moderna booster) and then waned to 46% at about 3 months.
Now, 74% protection against infection waning over 2-3 months to about 46% is not perfect. But it is not negligible either, especially when it comes to a virus that may cause serious long-term health consequences for those who get even mild acute infections.
And data from the C.D.C. shows that even after 5 months following a third (booster) shot, the Pfizer and Moderna vaccines remain about 78% effective against severe illness/hospitalization. Again, 78% protection is a drop from 91% during the first 2 months after a booster and it will likely wane further over time but this level of protection is still incredibly robust.
All of which is to say that if you have not yet gotten your booster shot, you do not yet understanding what is happening here–neither in terms of how great the current vaccines truly are nor in terms of what is at stake for your long-term health if you get C19.
What about second boosters (fourth shots)? We have fewer data to go on here but the available studies show limited but still favorable results. For example, this recent study in Nature Medicine demonstrates that the production of neutralizing antibodies against all variants goes up with each successive mRNA vaccine dose, offering higher levels of PASI. It is noteworthy that, with Omicron (and likely also with BA.2), those who received just 2 doses had virtually no neutralizing antibodies until they received the third shot, and also that a second booster (fourth shot) pushes neutralizing antibody titers even higher than after the first booster.

We also see that in older adults, neutralizing antibodies waned faster against Omicron than Delta, making it clear that, with the currently approved vaccines, booster shots are crucial to restoring VE against severe outcomes with the current variants. This would suggest that second booster shots are probably needed now. Note: the gray area represents the time during which the first booster shots were given.

Perhaps most importantly, using real-world data, the latest study from Israel shows that fourth shots of the Pfizer vaccine reduced the rate of infection by 2x and the rate of severe illness by 4x against Omicron among persons over 60 and those with compromised immunity.
Moderna has filed for EUA for a second booster dose for all adults, while Pfizer has applied similarly for EUA for a second booster for older adults. And the FDA is expected to announce soon that fourth shots will be made available as an elective to all adults over 50, although, moving into again new and strange territory, neither they nor the CDC are expected to issue any official guidance or recommendations.
Meanwhile, vaccination has ground to a halt in the US. We are one of the least vaccinated among advanced countries in the world and have one of the highest mortality rates to show for it. Many people, including some public health experts are falsely promoting the narrative that the vaccines have stopped working.
How should we be making sense of second boosters/fourth shots? Here’s my take: beginning today, Monday, March 28, in anticipation of the upcoming FDA announcement, we should begin to make available second boosters (fourth shots) of mRNA vaccine to anyone aged 50 and older who wants one. I’m going to take the shot and I’m going to take Moderna. Here are my reasons:
Vaccines do not completely eliminate the risk of getting infected but they significantly reduce it and a fourth shot/second booster lowers my risk of infection significantly.
Any symptomatic infection, even if illness is mild, can cause long-covid or organ tissue injury that may result in serious long-term health consequences. We now have 2 years of data to support this observation and there are no data that contradict it. I don’t want to have brain fog or chronic fatigue. I don’t want to not be able to taste food or suffer from chronic gastrointestinal distress. I don’t want to increase my risk for diabetes, kidney disease, dementia, and other chronic illnesses. And I don’t want my patients to have any of those problems either. So I will continue to promote boosters (and now, second boosters) to anyone who is interested in having that conversation.
PASI is most effective in the short-to-medium term (likely about 2-3 months) following vaccination. With another wave of cases expected in the next few weeks, that makes getting the second booster shot now seem like good strategy. Wastewater surveillance in San Diego shows a doubling of viral titers in just the last week (see below in Section III) so this seems like a good time to return our immune systems to a high state of preparedness.
Both mRNA vaccines offer protection but Moderna, probably because it uses a higher dose, offers a little more protection that lasts a little longer.
The Wall Street Journal, the Florida DPH, and Governor Ron Desantis disagree
On March 7, Florida Surgeon General Joseph Ladapo, who characterized C19 in children as a “trivial” disease, announced that “The Florida Department of Health is going to be the first state to officially recommend against the Covid-19 vaccines for healthy children.” Not that, as in the past, Florida would be taking a hands-off approach, ruling against vaccine mandates under the guise of so-called ‘medical freedom’ but rather that they are actually taking a position against childhood vaccination against C19.
And on March 20, the Wall Street Journal opinion section dedicated a substantial amount of print and video to promote the narrative that the pandemic is over and that the Biden administration needs to acknowledge it, stating, “The isolation has become it’s (sic) own pandemic.”
Meanwhile, a new study by the CDC shows that, during Omicron, the C19 incidence rates in Los Angeles County among unvaccinated persons were about 2 x higher compared to those who had received 2 shots of vaccine and 4 x higher compared to those who had received 3 shots. And the hospitalization rates among unvaccinated were 5 x higher compared to those who had received 2 shots and 23 x higher compared to those who had received 3 shots. During both Delta and Omicron predominance, both the case and hospitalization rates were highest among unvaccinated persons and lowest among those who had been boosted.
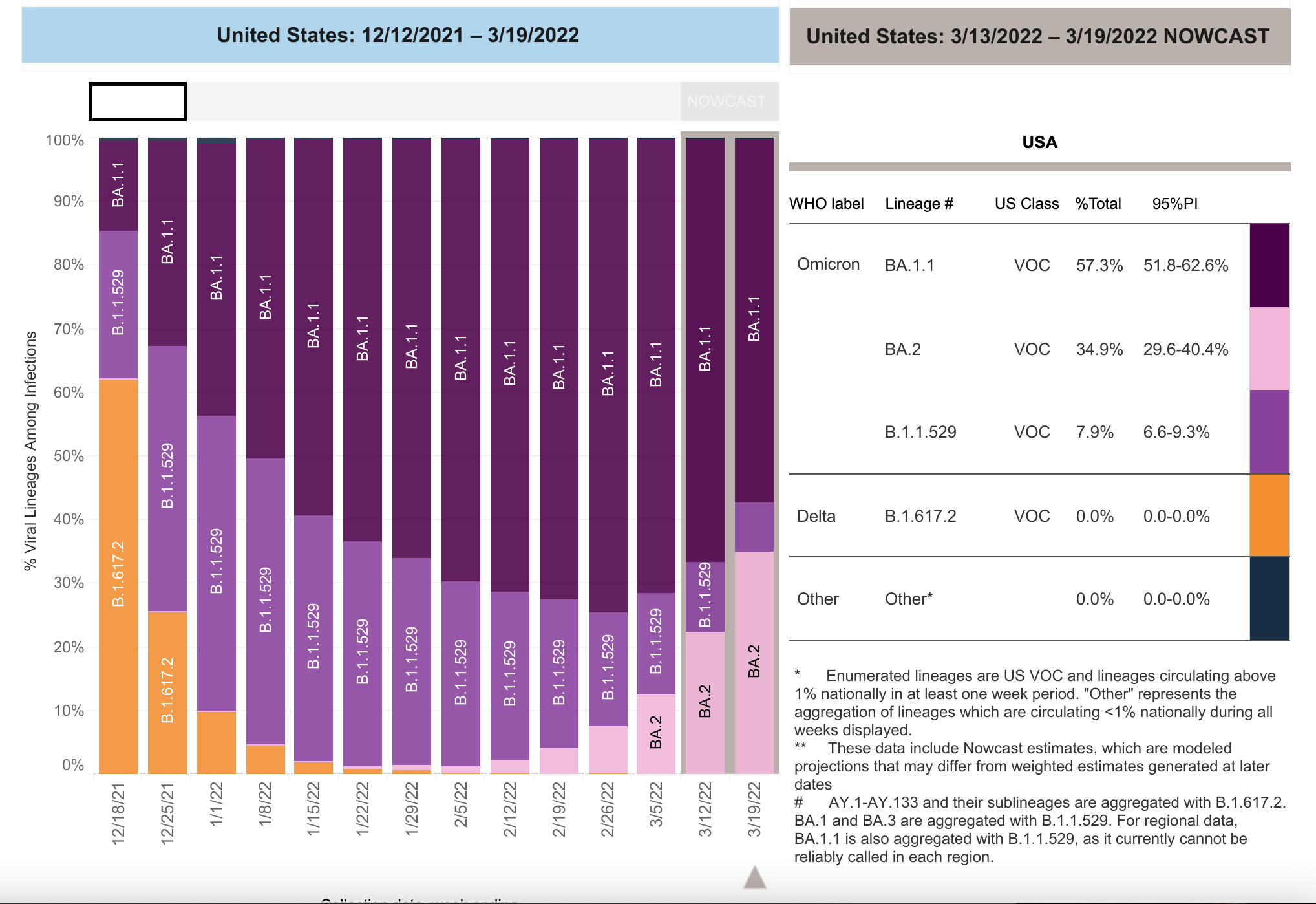
As discussed in the last Weekly Briefing, there is likely to be a new wave in the US in the next few weeks, driven by BA.2 which is on the rise in the US and will likely displace Omicron as the dominant variant in the next 2-3 weeks.
As previously discussed, there are some early data suggesting that BA.2 might be more virulent than Omicron, attacking the lungs more than Omicron did. And a new study in the Lancet shows that in a pediatric population, BA.2 is more virulent than prior variants (and more virulent than influenza).
Cases of BA.2 are rising quickly and now make up about 40% of all cases in the US.
So, as the Florida Department of Public Health, Surgeon General, and governor all pat themselves on the back for bravely advising against childhood vaccination, even in the light of an enormous body of data showing that children get long-covid and organ tissue injury that could impact their future health even after mild infections, I will continue to promote the non-political, fact-based narrative that says the opposite: parents, please get your kids protected against C19 as soon as possible.
III. The local scene
As reported last week, wastewater surveillance is showing dramatic upticks in Scov2 viral loads in over a third of the country, focused mostly in the northeast. Here, in San Diego, we saw a doubling of the amount of Scov2 virus in wastewater just over the last week. This has led UCSD to return to stricter anti-pandemic measures before the State of California mandates it, and that’s the right move.
Why not wait until the official case rate comes back up into the orange or red before putting the masks back on? Partly because there is so much less testing than there once was. Between non-testing and home, work, or school rapid testing (none of which is counted as part of the official case rate), the current case prevalence is now so underreported as to make that metric almost unusable. Wastewater surveillance is a better indicator of true community prevalence and the recent doubling over the last week is a sign that BA.2 is starting to take off in San Diego.
IV. Long-covid and organ tissue injury update (the effects of even mild infections on long-term health)
Despite the prevailing narrative that catching C19 is now an acceptable risk of normal life provided it doesn’t overwhelm the hospitals or result in an exceedingly high death toll, data continues to mount, week by week, showing that even mild cases are causing serious health problems down the road for those who get infected.
For example, this week, a new study shows that about 30% of healthy young people who get mild C19 infections develop peripheral neuropathy and that about 7% go on to have those symptoms last for up to 3 months. The authors conclude that these findings suggest that perpheral nerve injury takes place during (even mild) C19 disease and may have as-yet unknown long-term health consequences.
And in another new, high-powered study, researchers investigated the risks and burdens of new-onset (incident) diabetes and new use of antihyperglycemia (blood sugar lowering) medicines between three large cohorts: people who were infected with Scov2 over the last 2 years; those who were not infected by Scov2 over the last 2 years (contemporary control group); and those whose pre-pandemic electronic medical information were available for comparison (historical control group).
Those who had C19 exhibited a significantly higher risk of new-onset diabetes (28%) and new-onset use of antihyperglycemic therapies compared to both the contemporary and historical control groups. Even people at low risk for developing diabetes prior to contracting C19 exhibited increased risk after infection compared to both contemporary and historical controls.
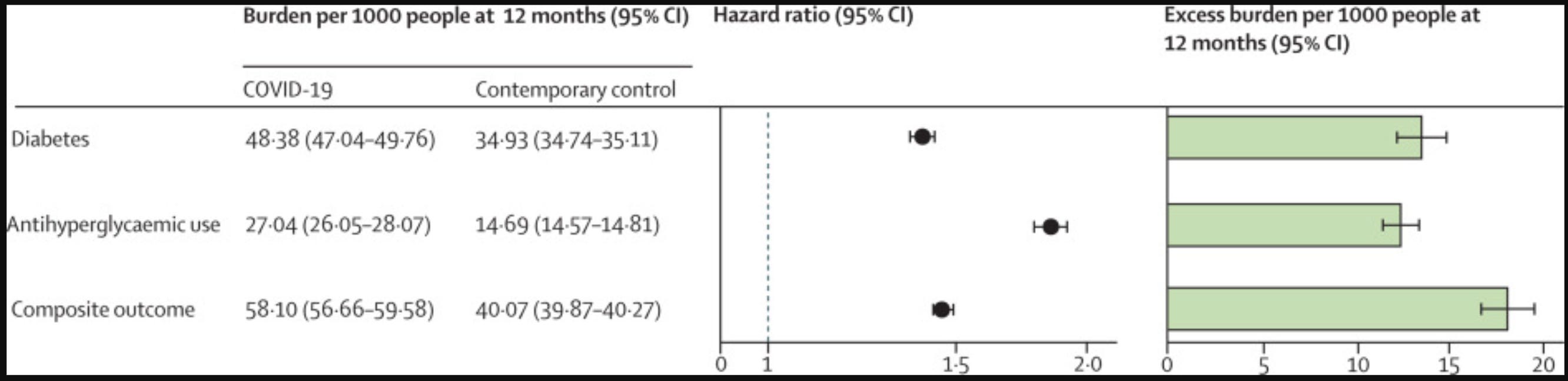
The excess burden of diabetes among non-hospitalized individuals was 8.3/1,000 people at 12 months post-infection. With an estimated 140M Americans having been infected so far, that number translates into an excess burden of about 1.2 M new cases if we extrapolate just from those who had mild infections. But the risks and burdens were even higher among those who were hospitalized, and higher still among those who received ICU care, so the true increase in incident diabetes caused by C19 infections is probably significantly higher than that.

The authors conclude that “diabetes should be considered as a component of the multifaceted long COVID. Post-acute care strategies of people with COVID-19 should also integrate screening and management of diabetes.”
Of course, we can add these new studies to the pile of data suggesting that the biggest story about the C19 pandemic may not be the astonishing excess death rate but the effect the virus will have on the long-term health of populations the world over, and the implications this will have in terms of already overburdened and underfunded healthcare systems, workforce productivity, and straining social safety nets–especially in countries like the United States, where recent estimates show that about10% of the population is without any health insurance.
The CDC has chosen its path, doubling and tripling down on driving a story that it is okay to get C19 so long as the hospitalization rates from acute infections do not overwhelm the healthcare system in the immediate term. This may turn out to be the greatest misstep in that venerable organization’s storied history.