

Covid and Long-Covid and Monkeypox, Oh My!
Updates and sensemaking about the pandemic and more

A Summer Plea To Colleagues, Patients, Friends, and Family
I. The Confusing State of Play
A few days ago, a close friend’s adult daughter tested positive for COVID-19. She had already been sick for a little over a week but was getting worse, not better, with a fever, productive cough, body aches, and headache. “She’s going to an urgent care in the morning, what medicine should she ask them for?” my friend wanted to know.
The antiviral therapies we have for the current dominant strain, known as BA.2.12.1, include Paxlovid, a combination of two medicines taken as pills twice a day for five days, and monoclonal antibody (mAb) therapy which is administered intravenously at a handful of approved mAb treatment sites. These therapies have been reserved for only those with mild to moderate COVID-19 (henceforth Covid) who are deemed to be at high risk for progression to severe disease. What’s more, they must be started right away–within the first few days of symptoms–for them to be effective.
So, in the case of my friend’s daughter, the fact that she had already been sick for more than a week would preclude her from being able to receive either intervention, even if she were in the ‘high risk’ category, which she isn’t. I explained to him that she would probably be told to take a fever and pain reducer like Tylenol or ibuprofen and to isolate until she had tested negative on a rapid antigen test (RAT) two days in a row (our office’s protocol). In fact, she was instructed by the urgent care physician to just return to work (as a hospital nurse!).
Yes, she was still sick, including a cough that was bringing up phlegm and getting sicker by the day. And yes, she was still testing positive on RATs which, by definition, meant that she was carrying high viral loads in her nose and therefore, was highly likely to be infectious. And yes, her work involves prolonged, close contact with other healthcare workers and patients already experiencing health problems serious enough to land them in the hospital. But she had been sick for more than five days and, according to the CDC, that is all the time required of a vaccinated person to isolate. Well, that’s what she was told anyway. Actually, the CDC guidelines (established at the end of last year) qualify that breaking isolation after five days should also involve an improving clinical picture with resolving or resolved symptoms (she was experiencing the opposite) along with masking for an additional five days.
Both the outdated CDC guidelines and the urgent care provider’s misquoting of them highlight the degree to which so many physicians and allied health professionals have been displaced from good sensemaking when it comes to virtually all things Covid. Should I bother getting tested? When should I test? Which test should I get? What does one positive test mean? Should I isolate? When should I break isolation? Ask five healthcare professionals these questions and you’re likely to get as many different answers. And that helps explain the current situation in which we find ourselves.
Confusing recommendations from the CDC that no longer track with what we are seeing clinically. Every business–including every medical office–doing something different. Public health policies that subserve a strategy of safeguarding hospitals from being overrun rather than preventing the spread of a disease whose long-term effects have not been established… Medical providers are busy taking care of patients, they don’t have the time or the bandwidth to master the ever-shifting landscape of this novel and complex disease. So how can non-medical providers know what is the right thing to do?
Here in San Diego, almost no one wears a mask anymore. The restaurants and bars are packed. Social gatherings have again become routine. Nearly everyone has internalized the false belief that you can’t catch Covid outdoors. PCR testing has become hard to find and is often prohibitively expensive, so most people are either using RATs or not testing at all. And since positive PCR tests performed by a certified lab remain the sole determinant of the daily case rate, that metric is now a gross underestimate of what’s actually happening.
The only reliable way to track the spread of Covid in a community now is through wastewater surveillance. As I have discussed at length in previous Briefings, monitoring sewage for SARS-CoV-2 does not provide us with a case rate but it can tell us if the amount of virus in a community is going up or down, by how much, and at what rate.

In this graph, we see that in San Diego, there is currently more virus in the wastewater (blue dots) than at any prior time during the pandemic excluding the enormous Omicron wave. There is now nearly three times the amount of virus in our wastewater as there was at the peak of the Delta wave last summer.
What’s more, the current wave has been rising steadily for more than three continuous months as ever more transmissible variants continue to take root, flower, and push out the old variants. This is a new phenomenon–a continuously building wave powered by multiple new variants. The Omicron wave was like a sprinter: a sudden explosion that was over relatively quickly. By comparison, the current wave–the product of four different variants–looks to be more like a distance runner: less explosive but with more endurance.
We also see in that graph, for the first time, a disconnect between the amount of virus in the community (blue dots) and the local case rate (orange line). In the past, the amount of virus in the wastewater typically began rising about two weeks prior to each new wave of documented cases but those metrics were closely tied to one another and followed nearly identical curves. But now, viral levels in the wastewater are climbing out of proportion to the case rate as fewer PCR tests are being performed and more people are using at-home RATs (or not getting tested at all).
In fact, public health experts estimate that, depending on where you live, the true case rate might be anywhere from 5 to 25 times higher than the reported rate. A national estimate of the current true case rate is about 8 times that of the reported rate. That means that, with a current national reported daily case rate of about 110,000, the real number is closer to a million new cases per day in the US.
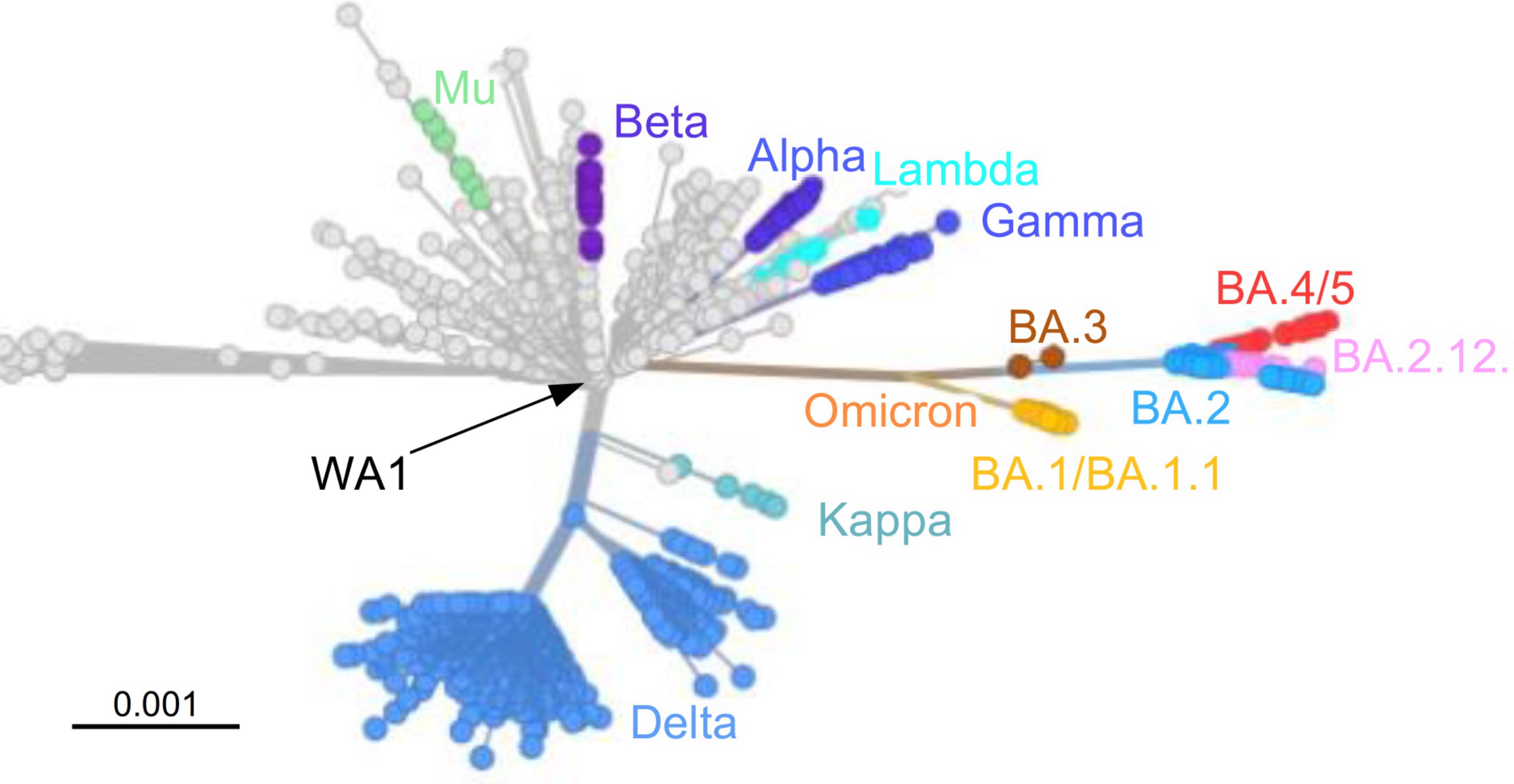
The public health department is not using the wastewater data and the CDC has not improved its now outdated messaging established at the beginning of the Omicron wave. It may be hard to believe but that was four variants ago. Omicron (BA.1) was replaced by BA.2 in February/March of this year. BA.2 was replaced by BA2.12.1, the current dominant variant, during April and May. And now we see two new variants, BA.4 and BA.5, strongly on the rise.
These last three variants (BA.2.12.1, BA.4, and BA.5) are each more transmissible than the prior strain (BA.2) which was more transmissible than Omicron (BA.1), which was more transmissible than Delta, which was more transmissible than Alpha, the variant that caused the first big wave in the US nearly two years ago.
And there is some evidence that these new, highly mutated variants may also be more virulent. While they do not seem to be causing higher rates of death or severe disease that would require hospital/ICU care, people getting infected with the new variants seem to be getting sicker, with more symptoms that are lasting longer. New research also shows that the new strains, all of which contain a particular mutation in the virus’ receptor-binding domain (called L452R), are also better at evading prior immunity, including the immunity provided from recent Omicron infection.
In this graph from Github, showing the different variants tracked over the last four months, we see in purple the virtual disappearance of Omicron (BA.1) and in light blue, the waning of BA.2. On the rise, we see BA.2.12.1 in red (the current dominant variant as of June 1), BA.4 in green, and BA.5 in yellow.

BA.5 has just taken root but is rising the fastest (as indicated by the steepest incline on the graph), followed by BA.4 (also a newcomer) and then BA.2.12.1. This could indicate that the current wave has yet a long way to go. Infections have already climbed much higher than was originally predicted when BA.2 was first identified.
In a nutshell, we are now on the upslope of the longest and at least the second-largest wave of the pandemic but somehow, no one seems to know it. People have stopped masking–even indoors. Even in Ubers and on airplanes. Congregate group activities including parties, festivals, concerts, trade shows, restaurants, bars, and classrooms are now about as common and as packed as they were before the pandemic. Employers like Elon Musk are requiring all employees to return to the workplace or be fired. Vaccination rates in the US are among the lowest in the industrialized world and the effectiveness of the vaccines is declining as each new variant migrates genetically further from the original wild-type strain against which they were built.
This also helps to explain why mAbs were working about as well against BA2 as they did against Omicron (BA.1) but are now losing their effectiveness against the new strains. A new study evaluating the sensitivity of BA.2.12.1, BA.4, and BA.5 against eight mAbs (bamlanivimab, bebtelovimab, casirivi mab, cilgavimab, etesevimab, imdevimab, sotrovimab, and tixagevimab) shows wide differences in the susceptibility of each variant to each mAb but the basic trend is toward more resistance.
II. Paxlovid Update
One of the biggest breakthroughs of the pandemic was the development of a new antiviral medicine called Paxlovid. Paxlovid was shown to be extremely effective (about 90%) at preventing severe illness and death among those most at risk of developing severe disease if used early in the infection. It is likely, at least in part, responsible for the lower Covid death rates that we are now seeing and, as it is finally becoming more available, there was hope that it might be used not just in patients who are most vulnerable to developing severe disease but more widely–for anyone in the first few days of symptomatic illness.
By knocking down viral loads, Paxlovid was expected to be effective at more than shortening the duration of illness and preventing progression to hospitalization and death. It was reasonable to assume it might also decrease transmission and lower the risk of Long-Covid and organ tissue injury seen commonly among younger, healthier people who get even mild acute infections. It was even hoped that it might be effective as prophylaxis.
Unfortunately, preliminary results from a new study conducted by Pfizer showed that Paxlovid does not seem to significantly reduce the risk of secondary infections. Prophylactic treatment with Paxlovid among 3,500 household members of people infected with SARS-CoV-2 did not significantly prevent the spread withing households compared to placebo. Will those who were treated with Paxlovid prophylactically but still got infected have less severe and/or shorter durations of illness? We will have to wait until the study has been completed. Will they have a lower rate of progression to Long-Covid? Will we find out down the road that these people had less damage to the heart, brain, testes, blood vessels, and kidneys? Only time will tell.
And Paxlovid has some other problems. Taking the medicine is not so easy on the body and many patients report significant side effects, including diarrhea, upset stomach, body aches, and dysgeusia (an abnormal and unpleasant sense of taste). Paxlovid is a combination of two medicines nirmatrelvir and ritonavir taken twice per day for five days. The purpose of ritonavir is to help prevent the degradation of nirmatrelvir which interferes with the ability of SARS-CoV-2 to make copies of itself.
Nirmatrelvir is bitter tasting, so keeping it active in the system may be part of what causes the unpleasant bitter grapefruit mixed with soap flavor that can continue even beyond the last dose, making eating most foods unpalatable. Stomach aches and diarrhea, well, that’s never pleasant. And while these side-effects were reported in a small percentage of subjects during the drug’s clinical trials, our office is noting them to be quite common among our patients prescribed Paxlovid.
More concerningly, during the clinical trials, it was noted that a small number of participants (1-2%) who received the drug got better, cleared the virus (tested negative) but then, days later, relapsed symptomatically and tested positive again–a phenomenon known as rebound infection or rebound Covid. But the real-world data might reflect a much higher percentage as we have also noted rebound Covid in many of our patients. Bob Wachter, head of the UCSF Department of Medicine and someone who I follow closely, conducted an online survey recently among those who had received Paxlovid, asking whether or not they had experienced rebound Covid and found that nearly half (45%) responded that they had.
Of course, surveys are often inaccurate and our experience with our patients might represent outlier data–the tyranny of small numbers, as data analysts like to say. But the journalistic and medical literature suggests that our experience is not unique.
Why is this happening and would I take Paxlovid if offered to me to treat Covid?
The Paxlovid clinical trials were conducted during the Delta wave before any of us had been vaccinated and that could be playing a role here. How? Vaccination creates immunity which can slow the rate of the virus’ growth inside the body. Add to that five days of nirmatrelvir which further inhibits viral replication and Paxlovid might in some cases be knocking SARS-CoV-2 down–but not out. Vaccination is protecting us from getting severely ill but it also appears, in some cases, to be prolonging the period of infection and infectiousness, so a five-day course of Paxlovid, which was sufficient before vaccination, may be too short now.
Delta was also a different variant that caused disease with a higher mortality rate but lower viral loads. The now dominant variant, BA.2.12.1, tends to cause much higher viral titers, so the current doses of nirmatrelvir and/or ritonavir in Paxlovid may be too low for the new variants in a growing number of cases.
I assume that Pfizer is conducting new clinical trials using longer courses and higher doses of Paxlovid and that we will hear about this soon. In the meantime, would I take Paxlovid to treat a Covid infection if I could? Yes. I’d deal with dysgeusia and gastrointestinal distress for five+ days if I was in the unlucky group who experienced such side effects. I would also spray Enovid (the antiviral spray from Israel that we stock at the office) into my nose five times per day to knock down the viral load in my upper airway. I’d sleep as much as I could and drink a lot of water. If I did not have a fever, I’d sauna bathe twice per day. We don’t know yet if Paxlovid decreases the risk of developing Long-Covid and/or organ tissue injury but it makes sense that lowering the viral load could be helpful in that regard and, as those of you who have been following my Briefings know, that is my chief concern regarding Covid.
III. Long-Covid Update
When the pandemic began, SARS-CoV-2 was quickly classified as a respiratory virus because the symptoms of Covid during the first wave of the pandemic centered on dry cough and difficulty breathing. In time, however, it became clear that Covid is more than just a respiratory illness. We learned that the virus is capable of infecting and injuring nearly every organ tissue including the testes, brain, heart, kidneys, fat, blood vessels, immune cells, and the gastrointestinal (GI) tract.
In a recent Briefing, I presented new data showing that the testes routinely sustain injury and scarring following even mild cases of Covid and could potentially be a reservoir for the virus for many months following acute infection. In other briefings, I presented data showing that men who got infected routinely experience significant drops in sperm count and sperm quality that in some may be long lasting and that men who got C19 seem to be experiencing erectile dysfunction at a much higher rate compared to those who have not been infected.
Over the last 20 years, the UK has been creating a database known as the UK Biobank Project, collecting in-depth genetic and health information from half a million volunteers. They run sophisticated blood tests, perform brain MRIs, chest CT scans and gather other data which they make available to medical researchers. In 2021, they recalled about 800 participants who had undergone brain MRIs prior to the pandemic–half who had had Covid and half who had not been infected–and rescanned them. They matched the two groups by age, sex, and comorbidities and found that for those who had been infected, regardless of whether they had experienced mild, moderate, or severe acute illness, part of their brain was now missing–the area that deals with smell, taste, and memory. This was not seen in any of the subjects who had not been infected and whose brains looked more or less identical to their pre-pandemic scans.
And in another study, disruption of microstructural and functional brain integrity was seen on diffusion tensor imaging–a special technique using MRI to track the movement of water molecules which can reveal microscopic details about the tissue architecture of the brain and spinal cord. The findings were correlated with neurological symptoms post-infection and the same brain areas of smell, taste, and memory were seen to be injured. The authors note that these findings suggest that there will likely be long-term brain health consequences among those who get even mild Covid.
One of the more common symptoms of Covid and one version of Long-Covid includes recurring bouts of nausea, vomiting, and/or diarrhea/GI distress. Data are now showing that one possible cause of Long-Covid with GI symptoms may be the persistence of the virus or an inability to clear bits of the virus (viral proteins) from the gut. In this study, approximately half of all people infected with SARS-CoV-2 shed viral RNA in their feces (which we are measuring in the wastewater), and about 4% of them continue to do so at least 7 months after having been infected. These people continued to have GI distress as part of their Long-Covid experience. The patients in this study all had experienced mild or moderate acute infections.
In another study using endoscopy performed on patients with inflammatory bowel disease (IBD) following Covid, SARS-CoV-2 antigen (viral RNA) and killer T cells directed toward the virus were detected in the gut mucosa for at least 7 months after mild Covid in about two-thirds of patients with IBD. Long-Covid symptoms were present in the majority of patients with viral antigen persistence, but not in patients without viral antigen persistence.
I recently reported on a study showing that about 30% of healthy young people who get mild Covid develop peripheral neuropathy and that about 7% go on to have those symptoms last for up to 3 months. The authors concluded that these findings suggest that peripheral nerve injury takes place during (even mild) Covid and may have as-yet-unknown long-term health consequences.
I also recently reported on a new high-powered study that showed that Covid survivors had a significantly higher risk of new-onset diabetes (28%) compared to both the contemporary and historical control groups, translating into an excess burden of about 1.2 M new cases of diabetes, so far, that can be attributed to Covid.
And now, in a new study from the CDC, we learned last week that Covid survivors have twice the risk of developing pulmonary embolism or respiratory conditions, and one in five adults under 65 and one in four aged 65 or older developed at least one serious chronic health condition affecting the brain, heart, lungs, musculoskeletal system, blood vessels, kidneys, or other organ systems that appear to be attributable to having had Covid.
The authors of the study conclude: “Implementation of COVID-19 prevention strategies, as well as routine assessment for post-COVID conditions among persons who survive COVID-19, is critical to reducing the incidence and impact of post-COVID, particularly among adults aged ≥65 years.”
It is noteworthy that they should emphasize prevention strategies for those 65 and over. I would push back against that (as I do against letting a nurse who is still testing positive to return to work). It is, in fact, more likely that children, teens, and young adults will be the ones most impacted by Long-Covid and organ tissue damage. The effects of chronic fatigue, depression, brain fog, early-onset dementia, pulmonary and heart disease, diabetes, and myriad post-covid conditions on the quality of life and workforce productivity is hard to predict but one way to quantify those losses is to multiply the degree of disability by the number of years these people are expected to go on living.
All of which compels me to recenter the Covid conversation, at least for this one Briefing, and to make a plea to take masking and other safety behavior seriously for a while longer.
Monkeypox: What is it and should we be worried?
I. The Illness
Monkeypox virus was first discovered in monkeys but is thought to be spread to humans mostly through contact with rodents. It’s a relative of the virus that causes smallpox (variola) and is endemic to parts of Africa. Monkeypox is an unpleasant and protracted illness that lasts several weeks but is generally less deadly than smallpox. Few healthy children and adults in the developed world who get Monkeypox will wind up hospitalized.
That said, there is some variation between the milder version of the virus found in Western Africa (West African monkeypox) and the more virulent strain found in Central Africa (Congo Basin monkeypox); West African monkeypox has a death rate of about 1% while the Congo Basin strain has a death rate of about 10%. Those numbers may sound high but most of the people living in those areas are impoverished and do not have access to first-world healthcare. The hospitalization rate in the US, should monkeypox spread more widely here, is expected to be very low and the death rate close to zero provided the current outbreak is being caused by one of these two known strains.
The virus enters the body by touching a contaminated surface (like a doorknob) and then touching one’s face. This is called fomite transmission. It is also spread during close contact through respiratory droplets (small saliva particles that fly a few feet through the air from people’s mouths when they speak) or when exchanging saliva such as with kissing or sharing food/drinks. This is called direct transmission. Luckily, monkeypox is not spread through airborne transmission, the way that Covid is. In terms of it contagiousness, monkeypox it is more like a cold or flu.
Monkeypox has a 10-14 day incubation period during which the virus builds up in the body before there are any symptoms. People with monkeypox are generally not contagious during the incubation period but can start spreading the disease once they become symptomatic. The most common symptoms include a flu-like illness (fever, body aches, headache, sometimes shortness of breath) followed 1-10 days later by a rash, often on the face/head, extremities, and/or torso that eventually turns into blisters filled with pus. The recent cases in Europe and the US have included some reports of lesions on the genitals as well. Symptoms usually last for 2-4 weeks and the skin lesions usually scab over in 14 to 21 days. People are generally considered to be contagious from the time of the onset of symptoms until their skin has healed.
II. The Virus and Vaccines
Unlike SARS-CoV-2 which is an RNA virus that mutates rapidly, monkeypox is caused by a DNA virus that mutates slowly. That means vaccination against monkeypox generally provides immunity that lasts a long time. Because it is a fairly close cousin of smallpox and thanks to an eradication campaign conducted around the world beginning in the 1950s, most older Americans have been vaccinated against smallpox and therefore, have some protection already against monkeypox. However, that campaign started winding down in the 1970s and was discontinued in 1980, once smallpox was essentially eradicated from nature and no longer considered a threat. That means that young Americans are mostly unvaccinated against smallpox and therefore, have no protection against monkeypox either. Prudently, the US government stockpiled a fairly large amount of smallpox vaccine just in case the virus reappeared. We also have stockpiles of another vaccine (called Jynneos) that is tuned to both smallpox and monkeypox.
Although historically mostly isolated to Africa (especially The Democratic Republic of the Congo and Nigeria), there was a reported outbreak of monkeypox in the US in 2003, when a shipment of rodents from Ghana spread the virus to pet prairie dogs in Illinois which in turn infected more than 70 people in the US. That outbreak was contained using a technique called ring vaccination which involves immunizing the close contacts of people who have been infected to cut off any routes of transmission. In addition to stockpiles of vaccines, we also have antiviral treatments thought to be effective against the virus.
III. The Next Pandemic?
The CDC is keeping a close watch on monkeypox and right now, there is no reason for panic. If the numbers continue to grow, it is likely that ring vaccination would again be employed to contain the spread. The current outbreak is still relatively small with about 257 confirmed cases in 11 countries outside of Africa so far, including 9 cases in 7 states in the US. Most of the cases are among relatively young gay and bisexual men who have sex with other men. It is probably being spread by close contact within those social/sexual communities.
Covid is a novel disease for which almost no humans had prior immunity. It is also an airborne disease which accounts, in part, for why it is so astonishingly transmissible. It can be spread before a person knows that they have it (during the incubation period) and by people who are infected but asymptomatic. These too add to Covid’s extremely high transmissibility. Because it is an RNA virus that mutates rapidly, SARS-CoV-2 can spawn new variants every few months capable of evading prior immunity. These are some of the factors that led to and continue to fuel the current pandemic but none of them pertain to monkeypox. In short, it is unlikely that monkeypox will blossom into an epidemic or pandemic. That said, this would all change if the current outbreak is being driven by a new and more transmissible variant of the virus, so stay tuned…