

Dr. Berkoff's Health Science Briefing for April 25, 2022
Advances in the treatment of depression; the gut microbiome is like an organ and may even play a role in long-covid; and vaccines against cancer?

First, some general housekeeping: As I continue to expand the Briefings to include a more diverse assortment of health-related topics, and with my clinical chiropractic practice now back in full-swing, going forward, I will no longer be publishing on a weekly-basis. Rather, the Briefings will be published as time permits for the completetion of each installment. Time-sentitive COVID-19 ‘Mini-Briefs’ may be issued from time-to-time on an as-needed basis. I have also changed the name to reflect the wider array of subject matter being addressed.
This Briefing begins with an interesting new clinical study on depression. Last week we were privileged to have psychiatrist Dr. Dmitriy Sivtzov perform an in-service at the clinic on the latest advances in the treatment of major depressive disorder (MDD), including a review of transcranial magnetic stimulation (TMS), and ketamine and psilocybin-assisted psychotherapy (PAT).
Last week, a new (small) randomized clinical trial provided the first hard data on the efficacy of PAT for the treatment of major depression. The study demonstrated a rapid (within one day), lasting (at least one-month post-treatment), and significant (more than 50% reduction in symptoms among two-thirds of patients and complete remission among one-third) improvement in symptoms of major depression following PAT.
These findings support the use of psilocybin with traditional therapy as an effective intervention for MDD, consistent with Dr. Sivtzov’s clinical experience.
What is the Gut Microbiome and why is it important?
I. There are a lot more of them than there are of us
The gut microbiome or the microbiota refers to the trillions of invisible microorganisms that live within our intestines. In the image below, taken from Dr. Erica Sonnenberg’s lecture at the Stanford Center for Clinical Research, which can be found here, the pink and yellow dots represent microorganisms living in the colon (the images presented below, except as otherwise referenced, were taken from this lecture). In blue are the cells that form the colon wall (also called mucosal cells or mucous membranes). And in green, we see the mucous that is secreted by those cells which creates a protective barrier against infection by those microorganisms.

Close to a hundred trillion microorganisms reside within a healthy human intestinal system, including bacteria, fungi, yeasts, viruses, and bacteriophages (specialized viruses that infect bacteria).
When I was doing my training more than 30 years ago, we did not know that these microorganisms are as deeply integrated into the function of our biology as we do today. Currently, most experts view the gut microbiome (GMB) as another organ–one that profoundly influences many aspects of our health, including metabolism, immunity, mood, and brain function.
Because of the staggering number of microorganisms in the colon, there are about one hundred times more genes in the GMB than there are in the human genome. And we benefit from these genes in many ways. The ability to sequence not just particular genes but whole genomes of the many species of microorganisms that live in the GMB, through technological innovations like shotgun metagenomics, has revolutionized our understanding of the degree to which we live in symbiosis (a mutually interactive and beneficial relationship), genetically and biochemically, with the microorganisms that have colonized our gut.
And the same thing is going on in our noses, mouths, throats, and vaginas, and on our skin–albeit with some significant species’ variation between each of these different microbiome compartments.
In a sense, one could say that we humans are like superorganisms, functioning to a substantial degree at the genetic direction of armies of microorganisms that have taken up residence on and within us, of whose presence we are as unaware as we are of our liver or kidneys.
When microorganisms such as the bacteria living in and on our bodies eat, they produce waste products called metabolites. It is fair to say that we not only make use of these metabolites, but we need them to survive and thrive. Which species’ of bacteria and metabolites are dominant varies according to the body area as different parts of the body require different metabolites to assist in performing specific local functions. But the GMB is the body’s most diverse and abundant microbiota compartment and it plays the greatest role in our overall health.
II. How does the GMB form?
(For a more in-depth discussion, please see Dr. Susan Lynch’s lecture at UCSF Grand Rounds which can be found here).
We are born with a very simple GMB laid down in the womb, and then rapidly accumulate new microorganisms as we come into contact with them through eating, drinking, breathing, and touching, over the first few years of life, typically establishing a more or less fully developed baseline microbiota by around age three.
However, this baseline early childhood GMB represents more of a general outline compared to the fully fleshed-out adult version, and the physiological effects of our microbiota evolve over time as well in response to various selective pressures including our diet, the amount of contact we have with dirt, the use of antimicrobial agents (like antibiotics and hand sanitizers) and other common medicines (like statins and metformin which are used widely to prevent or treat cardiovascular disease and diabetes, respectively).
Why? Certain foods, hygienic practices, and medicines are capable of decimating some microbial species and/or promoting the excessive growth (blooming) of others, throwing the GMB out of balance. We refer to this as GMB dysregulation or dysbiosis. When medicines, practices, and poor diets alter the composition of the GMB for the worse, they induce harmful changes to the composition of genes and metabolites available to us (more about this later).
Such selective pressures can even alter the way in which our bodies respond to certain medications. For example, the effectiveness of digoxin, a medicine used to treat heart failure, depends largely on the integrity of the GMB. If the GMB has been dysregulated, it may contain an overabundance of certain bacterial species’ which produce metabolites capable of inactivating it. Why do medicines work better on some people than on others? One reason is that dysregulated GMBs can interfere with their pharmacokinetics (how the body interacts with a drug).
III. How we benefit from our GMB–the symbiotic relationship
The human genome encodes for the ability to easily digest simple carbohydrates (sugars) but not complex carbs that contain a lot of fiber. It is only through the fermentation of fiber by gut bacteria that many important metabolites required for optimal health are produced.
Sugars of all kinds can be pulled right through the linings of the gastrointestinal tract into the bloodstream without much digestive processing, and starches (simple sugars linked together into long chains to technically form complex carbs that nevertheless lack fiber), including foods made from flour (with the exception of nut flours), are quickly broken down (digested) by pancreatic enzymes into sugar in the small intestine for easy absorption.
But, for most of human evolutionary history, sugary and starchy foods were rare and comprised only a very small percentage of total calorie consumption. Even when ripe fruits were briefly available in the summer months, these plants also contained plenty of fiber. And in order to digest fiber, we need assistance.
That assistance comes from the GMB. When fiber-loving bacteria in the GMB feed, they not only produce critical metabolites which we need for our own health but also induce the production of the mucous that protects us against infection by all those other microbes in our gut. In order to produce enough mucous to form the critical protective barrier that coats the intestinal mucosal cells, we need robust populations of fiber-loving bacteria and a steady and plentiful supply of indigestible dietary fiber to keep them alive.
Over time, the standard American diet (SAD), which is rich in fat and simple carbs but low in fiber and other complex carbs, leads to GMB dysbiosis. Sugar-loving bacteria overgrow (bloom) while the fiber-loving species’ are starved and eventually die off. Sugar-loving bacteria not only push out the mucous-producing, fiber-fermenting bacteria, they actually feed off the mucous itself (as well as sugar) leading to a thinning of the protective mucosal barrier.
Making things worse, the mucosal cells that line the colon contain some complex carbohydrates of their own. These complex carbs can be cannibalized by fiber-fermenting bacteria when there isn’t enough fiber in the diet. When fiber-loving bacteria break through a thinned-out mucous barrier and begin attacking mucosal cells to eat their stored complex carbs, this causes bowel inflammation.
So the SAD which is low in fiber and high in sugar not only leads to a reduction in the production of important metabolites that we need to survive and thrive and reduces our protection against infections by causing a thinning of the protective mucous barrier, it also promotes intestinal inflammation, something we refer to clinically as inflammatory bowel. A global survey published in Gastroenterology in 2021, using data from more than 73,000 adults from 33 countries, found that more than 40% of respondents had chronic symptoms consistent with gastrointestinal disorders like inflammatory bowel disease (IBD) or irritable bowel syndrome (IBS), including bloating, stomach discomfort, and recurring or chronic diarrhea and/or constipation.
In short the SAD is one of the least healthy diets in the world and our population-level health metrics reflect it. The US has the highest rate of chronic disease burden of any advanced country in the world.
Back to digestion
As previously mentioned, the human genome does not encode for the ability to digest complex carbs like fiber. When we eat fiber-dense foods like black rice, broccoli, beans, lentils, farro, and other high-fiber plant foods, indigestible fiber makes its way through the stomach and small intestine all the way to the colon (the large intestine) mostly intact. Once that fiber enters the colon, it becomes food for fiber-loving bacteria.
As these bacteria consume the fiber through fermentation, they release metabolites such as short-chain fatty acids (SCFAs), like acetate and butyrate, which help our bodies to regulate blood lipids and keep our body tissues sensitive to insulin (the hormone that regulates blood sugar levels). And recent research shows that butyrate, along with another SCFA released during bacterial fermentation of fiber called pentanoate, may help to fight cancer by strengthening the activity of specialized (killer) T cells–the part of our immunity that attacks infected cells and cancer cells.
IV. What does a healthy GMB look like?
As described beautifully in The Good Gut (Taking Control of Your Weight, Your Mood, and Your Long-Term Health) by, Justin and Erica Sonnenburg, perhaps the most important feature of a healthy GMB is diversity. Healthy people with stable blood sugar levels and low amounts of central or visceral fat (fat stored in and around our internal organs) tend to have highly diverse GMBs with several hundred different species of bacteria coexisting in the colon. By contrast, less healthy people with obesity and high blood sugar tend to have far fewer bacterial species in their GMBs.
As human diets have changed over time, from paleolithic hunter/gatherer societies, through the agricultural revolution, to the mass production of food, until the present day with the SAD marked by highly refined simple carbohydrate-dense, processed foods, manufactured to be delicious and addictive, we can trace a progressive ‘narrowing’ of the human GMB, with less and less diversity of bacterial species’ over time–at least among developed countries.
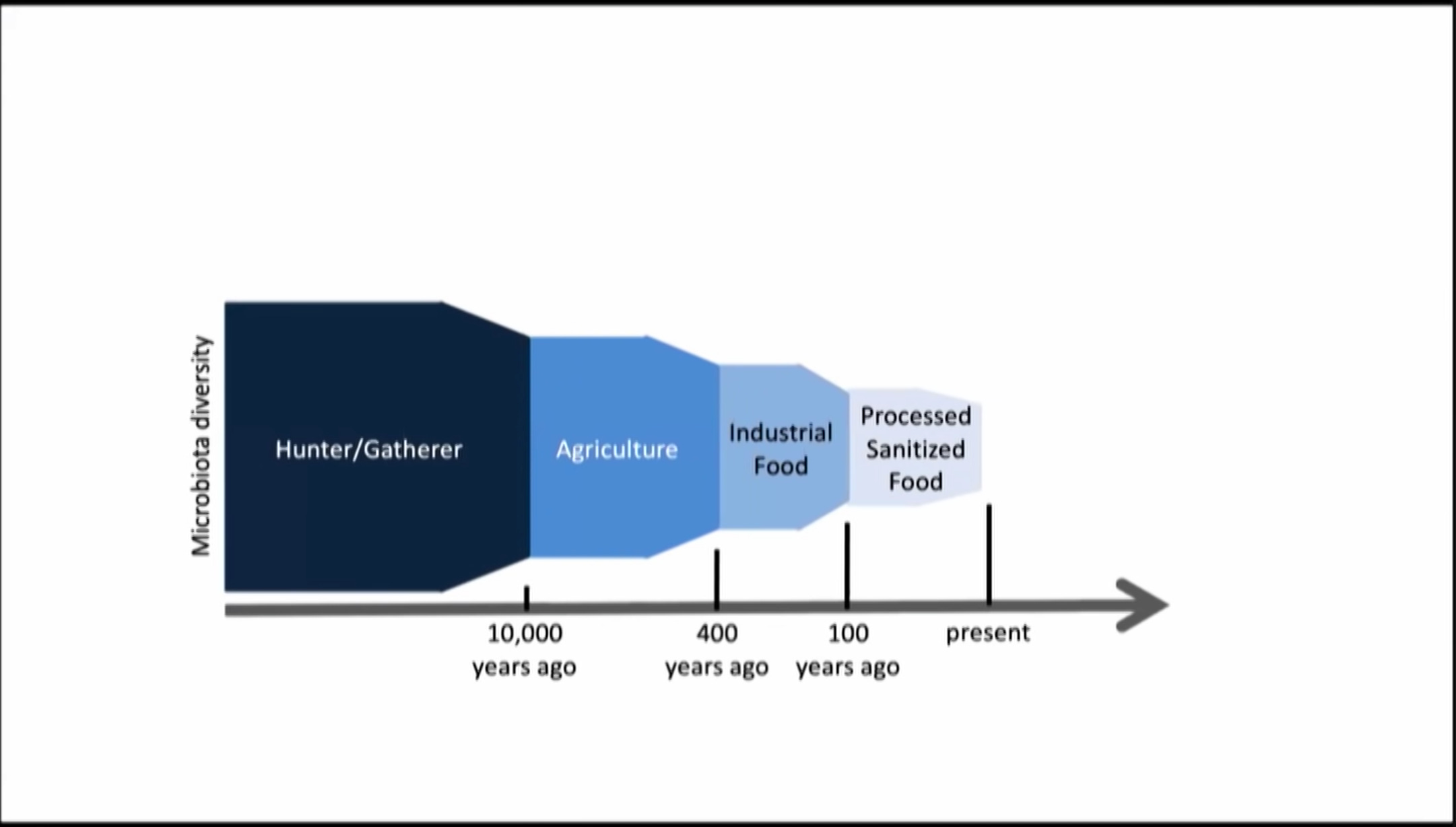
This helps explain why humans in industrialized nations today have more obesity, heart disease, and diabetes compared to humans living in most of Africa and parts of South America, where diets more closely resemble those of their ancestral hunter/gatherers.
For most of evolutionary history, human diets were rich in fiber and extremely low in sugar and flour. This enabled the development and maintenance of diverse and robust GMBs. But the SAD and similar diets among our industrialized counterparts have caused our GMBs to shrink and become less diverse. And now we are saddled with the enormous problem of having to deal with the health, productivity, and financial costs of that shift.

V. Back to Type-I Diabetes
For example, in a recent Briefing, I wrote about how industrialized countries are experiencing escalating rates of various autoimmune diseases, including Type-I diabetes (T1D). Finland now has the highest rate of T1D in the world. Meanwhile, just next door in Karolinska, Russia, where infants and children have a much higher exposure to dirt (and the microorganisms contained therein) and are far less likely to be treated with antibiotics during infancy and childhood, T1D is remarkably low. These two populations share the same weather, geography, and ethnic/genetic heredity.
What is driving the staggering difference in the rates of childhood T1D between these populations? Exposure to pathogens helps train our young immune systems to grow strong and function efficiently. It is thought that a lack of exposure to germs may lead to weakened immunity and various forms of immune dysregulation including autoimmunity.
Recent research now shows that an underdeveloped or dysregulated GMB in infants and young children is a key determinant of T1D with the decimation of bacterial species that produce SCFAs as the critical driver. Lack of exposure to key microorganisms found in dirt combined with high use of bacteria-killing antibiotics is causing the rates of T1D in Finland (and elsewhere) to soar.
VI. Allergies, asthma, depression, and more…
And the same framework applies to the development of many other forms of chronic illness. Allergies, autoimmune conditions like celiac disease (an inflammatory reaction to gluten, a protein found in wheat), and asthma appear to be responses to GMB dysbiosis. We now see strong relationships between GMB dysregulation and the development of psoriasis, autism, and psychiatric illness including depression. Even preterm birth can be predicted by the lack of a particular bacterial species (lactobacillus) in the vaginal microbiota of expectant mothers.
How do we know that dysregulation of the GMB is the driver of these diseases rather than the product of them? New data using mice raised in a sterile environment who have no GMB of their own have shed some light on the subject. In a groundbreaking study, germ-free mice raised in a sterile environment had their colons implanted with fecal material from either obese or healthy non-obese humans. Fecal material contains a cross-section of the GMB of the donor and, over time, the mice implanted with feces from obese humans developed a low diversity GMB that reflected the obese donor and these mice quickly became obese themselves. But mice implanted with feces from healthy non-obese humans developed highly diverse GMBs that reflected their healthy donors, and stayed lean despite being fed the same diet and the same number of calories as the group implanted with feces from obese donors!
It turns out that the dysregulated low-diversity GMBs of obese humans, containing an overgrowth of sugar-loving bacteria and diminished fiber-fermenting, mucous-producing bacteria, have an increased capacity to harvest energy from food compared to those with healthy, diverse GMBs, and this leads to weight gain.
Many similar studies on animals and humans have subsequently confirmed that GMB dysbiosis drives not only obesity but many other common chronic diseases. In a previous Briefing, I discussed how slowing metabolism in the context of a calorie-rich SAD can lead to obesity. But obesity is also driven in part by a shift in the composition of the GMB in response to the prolonged selective pressure of a diet that is high in sugar and starch and low in fiber.
VII. Fecal microbiota transplantation in humans
Fecal microbiota transplantation (FMT) refers to the transplantation of the GMB from healthy donors to patients. FMT offers the potential to revolutionize the treatment of many diseases through the restoration of dysregulated GMBs and has already yielded stunning therapeutic results across a wide array of human ailments.
One recent study in which FMT was used to treat children with autism spectrum disorder (ASD) is worthy of particular note. In this open-label clinical trial, FMT was found to be both safe and effective for relieving gastrointestinal and behavioral symptoms in children with autism by restoring their GMB. Participants with ASD were split into two groups: one which received oral capsule administration and one which received intra-rectal implantation of the same dose of a bacterial cocktail distilled from the feces of a healthy donor. Treatments were once a week for 4 weeks. The control group of neurotypical children (children without ASD) did not receive the bacterial cocktail. FMT, either through oral administration or implantation, not only led to a rapid and substantial reduction in GI and neurological/behavior symptoms associated with ASD, the relief was generally long-lasting. Children with ASD are known to have an imbalance in their profile of neuroregulatory hormones and this too was improved following FMT. It is worth noting that a review of medical records showed that the ASD cohort (the children with autism) had received about twice the number of courses of antibiotics during infancy and childhood compared to the non-autistic controls.
VIII. Fiber vs. fermented foods vs. probiotics
The human genome evolves slowly. Genetic mutations (which drive evolution) take place when living things reproduce and the time between human generations averages about 20 years. By contrast, bacteria in the GMB reproduce about every 20 minutes. That means that while we cannot, within our lifetimes, change our own genome, we can change our microbiome both compositionally and evolutionarily. And we can see changes rather quickly (within a day or two) simply based on what we choose to eat.
Unfortunately, our GMBs don’t change permanently after just a couple of days of eating a healthy, low-sugar, fiber-rich diet. They have ‘memory’ and after establishing and living with dysbiosis for years or decades, our bodies tend to want to come ‘home’ to that state of low-diversity dysregulation. It can take several years of a diet low in sugar and starch/high in fiber to establish a healthy, robust, diverse GMB as a ‘new normal.’ And even then, we may need a little extra help in the form of fermented foods (more about that below).
But temporary shifts can take place almost immediately and this can initiate a shift toward better health. In one of the best animal studies to date, switching humanized mice (mice raised in a sterile environment and then given FMT from a human donor to establish a ‘human’ GMB) from a low-fat, fiber-rich diet to a low fiber/high-sugar and fat SAD, shifted the structure of the microbiota within a single day, altering GMB gene expression and causing those humanized mice to become obese quickly when maintained on that diet.
Fiber
Perhaps the most important human (prospective) study to date comparing the effects of high fiber and high fermented food diets, showed that the group who were switched from a SAD to a high-fiber diet increased their nutrient profile and expanded the size (although not as much the breadth) of their GMBs, developing over just a few months many more bacteria and slightly more bacterial species’ capable of digesting fiber. These altered GMBs released fewer toxic metabolites and more healthful ones.
In addition, subjects who began the study with at least a moderate breadth of bacterial species’ (moderate or better GMB diversity) showed a significant lowering of inflammation. However, those who started the study with low bacterial diversity actually showed an increase in inflammation when moved to a high-fiber diet as the sole intervention.
Fermented foods
The group that was switched from a SAD to a high-fermented food diet (yogurt, kefir, kimchee, sauerkraut, etc.) demonstrated an even stronger increase in biodiversity in their GMBs, steadily increasing the number of different bacterial species by 25% over the four-month study period. In addition, all the participants in this group showed a lowering of inflammation.
Interestingly, it turned out that just a few (about 5%) of the new microbes found to have taken root in the GMBs of this group came from the fermented foods themselves; most (95%) of the new species did not come directly from the fermented foods that they ate. It appears that fermented foods expand the breadth (increase the diversity) of the GMB by making it more generally friendly to the process of colonizing new species.
Studies like these strongly inform my current perspective on what makes up an ideal diet. Today, I try to have a big serving of fiber and some probiotic-containing fermented food every time that I eat. Even when I ‘break bad’ and have a burrito, I open it up first and add yogurt or sour cream (for their active cultures) and typically have it with some roughage (like a side serving of black rice). I occasionally enjoy a pasta dish or a slice of pizza, but I try to take these meals with a big salad and/or some vegetables and add a little kombucha to my sparkling water to drink.
Probiotic pills
One would expect, based on the data from the fermented food cohort of the previously described study, that taking probiotic pills, which can deliver many more healthy bacterial species into the gut than a serving of fermented food, would have a similar or perhaps even stronger effect on the GMB (and our health) than those who added copious amounts of yogurt and kimchi to their diets.
But in fact, in another (double-blinded, placebo-controlled) study conducted on patients with metabolic syndrome, no improvements in GMB size or diversity were seen, nor was there any reduction in inflammation or any improvements in blood lipids, blood sugar, or insulin levels after taking probiotics. Patients with metabolic syndrome, on the whole, did not seem to benefit at all from high doses of probiotic supplements.
On deeper analysis, within the treatment group (but not the control group who did not have metabolic syndrome), about half of the patients given probiotics showed a worsening of inflammation, triglycerides, and blood sugar while the other half did show some benefit.
What was the difference between those made slightly worse and those who reaped a small benefit? Unlike in the prior study, where the differentiating factor between those who showed increased or decreased inflammation after being switched to a healthy high-fiber diet was their baseline GMB diversity, in the probiotic study, what made some patients respond to the treatment was that these ‘responders’ had more fiber in their diet while they were taking the probiotics.
IX. Lifestyle is the key
It is now clear that we can train our GMBs through dietary interventions to achieve better health. Diets rich in fiber (fruits, beans, whole grains, vegetables, etc.), especially combined with regular consumption of fermented foods, put positive selective pressure on our GMBs, causing them to evolve to look more like those of our ancestral hunter-gatherers. The benefits of supplementing with probiotic pills are likely to be small if accompanied by an ideal diet and non-existent or even harmful in the context of a SAD. I used to take and promote the use of expensive probiotic pills in my practice. I don’t take or sell them anymore.
Bearing in mind the concepts of GMB memory and resiliency, when we set about changing our diets to improve our health through diversifying the microbiota, we need to set our sites on making permanent changes to the way that we eat. For most of us, changing our diet to improve our GMB can only be maintained so long as we continue to eat healthily for several years. Slipping back into the old patterns of regularly consuming processed, starchy, sugary foods after just a few weeks or months of healthy eating will quickly return the GMB to its prior state of dysfunction, significantly impacting our health.
A side note about ketogenic (keto) diets: Keto diets, such as Atkins, which are comprised almost exclusively of fat and protein, have become progressively more popular over the couple of decades. They have been used successfully for weight loss and for the treatment of metabolic syndrome and diabetes. Keto diets offer significant health benefits. By virtually eliminating sugar and starch, keto diets keep blood sugar very stable and allow body tissues to become can contain little to no simple carbs so, unlike the SAD, they do not cause sugar-loving bacteria to bloom and take over the GMB. So far, so good.
However, since keto diets are also very low in fiber, they can cause the GMB to shrink and, as species of bacteria that survive by fermentation of fiber are deprived of their food, they can promote bowel inflammation and eventually even die off, making the GMB less diverse (more dysregulated) and allowing sugar loving bacteria to become more dominant.
In addition, it has not yet been established whether keto diets are successful at promoting weight loss because they tilt metabolism toward fat-burning (ketosis) or whether, because they are so restrictive in terms of what people following them are allowed to eat, that they indirectly result in calorie reduction due to auto-satiation (there is only so much fat and protein a person can eat before getting sick of it and naturally eating less food over time).
And, as discussed at some length in an earlier Briefing, prolonged calorie-restriction diets result a slowing of metabolism which is bad for our long-term health. For these reasons, I recommend that patients who are on or are interested in trying a keto diet, do so only on a short-term basis.
COVID-19 Science Updates
The gut microbiome (GMB) and long-covid (LC)
In a new prospective study of 106 patients with C19 (of varying severity) and 68 controls, serial microbiome analyses using shotgun metagenomic sequencing, demonstrated that at 6 months, 76% of patients had developed symptoms of LC including fatigue and memory loss that was predicted by GMB dysbiosis at the time of admission, characterized by higher levels of two particular sugar-loving bacterial species: Ruminococcus gnavus and Bacteroides vulgatus; and lower levels of one fiber-loving species: Faecalibacterium prausnitzii.
Patients who did not develop symptoms of LC had normal GMB profiles at admission and also at 6 months, comparable to that of non-C19 controls. And having high levels of fiber-fermenting, butyrate-producing bacteria (like Faecalibacterium prausnitzii) showed the strongest inverse correlations with LC at 6 months (the more of it that patients had, the less likely they were to develop LC).
These findings beg the question: can we prevent or treat LC with high fiber/high fermented food diets?
Probiotics improve outpatient C19 outcomes
In a new perspective quadruple-blinded study, patients with acute C19 were given either a probiotic cocktail or a placebo. By the end of the study, the treatment group had nearly double the rate of complete resolution of symptoms compared to the placebo group. Probiotic supplementation was well-tolerated and significantly reduced viral load, lung infiltrates, and the duration of symptoms, while increasing the production of antibodies against the SARS-CoV-2 virus, compared to placebo.
No significant compositional changes were detected in fecal microbiota between the probiotic (treatment) and placebo groups, leading to the assumption that the probiotic primarily acts by interacting with the host’s immune system rather than changing microbiota composition.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8757475/
Americans lost the most from C19 in terms of life expectancy
A new study demonstrates that average life expectancy (ALE) in the US in 2020 dropped by almost 2 years as a result of the pandemic, driven most extremely by the very high death rates among black and Hispanic Americans. Compared to our peers in the industrialized world, the US experienced by far the largest reduction in ALE.
The specific data: between 2019 and 2020, US ALE decreased by a mean of 1.87 years with much larger decreases in the Hispanic (3.70 years) and non-Hispanic Black (3.22 years) populations than in the non-Hispanic White population (1.38 years). The mean decrease in ALE among peer countries was 0.58 years across all 21 countries. No peer country experienced decreases as large as those seen in the US. Can we relate this, at least in part, to the standard American diet (SAD) and its effect on the gut microbiome (GMB)? It’s a reasonable hypothesis.
Finally, a diagnostic breakthrough for COVID-19 (C19)
With community ‘case rates’ based solely on positive PCR tests now representing an entirely unreliable metric for estimating C19 community prevalance and wastewater data being hard to access, we are now left with virtually no tools from which to make risk assessment.
Last week, the FDA has announced emergency use authorization (EUA) for a new breathalyzer test called InspectIR COVID-19 Breathalyzer which can detect the presence of volatile organic compounds (VOCs) produced by SARS-CoV-2, the virus that causes C19.
It was validated in a large study of more than 2,400 people including those without symptoms, and was shown to be 91% sensitive (the percent of positive samples the test correctly identified as confirmed by PCR testing) and 99% specific (the percent of negative samples the test correctly identified).
The study also showed that in a community where only 4.2% of the population have C19, the test had a negative predictive value of nearly 100%, meaning that people who receive a negative test result in the context of low community prevalence can rely on the test to be quite accurate, including against Omicron.
The instrument uses gas chromatography-mass spectrometry (GC-MS) to detect five VOCs associated with the virus in exhaled breath. Patients breathe into a single-use disposable straw–about enough air to fill a small balloon– and the unit makes the analysis in about three minutes. Then, the unit superheats the chamber containing the sample to sanitize it.
This is the innovation that our practice has been waiting for. No more swabbing the throat and nose, extremely fast turnaround times (three minutes to result), no pain or discomfort for patients, and the potential to move toward a mask-free office again. We are trying to purchase a unit for the practice.
Vaccines to prevent cancers
One of the good things to come out of the pandemic was the leap forward in mRNA technology that led to the miraculous success of the Moderna and Pfizer vaccines against C19. It has long been a dream to develop vaccines against not just infections but also cancers. And we have made some progress in that regard. Some viruses promote cancer and vaccines against viral infections have indirectly reduced the rate of certain cancers. For example, the HPV vaccine has indirectly reduced the rate of endocervical cancer.
But progress in developing vaccines to promote immunity that attacks cancer cells directly has been slow. Now, however, we are beginning to see some light. One new approach involves the targeting of “neoantigens,” a type of protein found only on cancer tumor cells. Some of the new anti-cancer vaccines deploy just a single neoantigen whereas others use several in an attempt to broadly shield against cancer. The best approach is unclear, and developers also face the difficulty of having to wait decades to see whether or not healthy people who receive the vaccines develop cancers. Worth a read: