

Dr. Berkoff's Health Science Briefing for May 2, 2022
Fasting vs. 'intermittent fasting'; depression medicines work mainly by the placebo effect; new approaches to antidepressant therapy; and how depression may impact fetal brain development.

Fasting is healthy; intermittent fasting less so…
This Briefing begins with a new study published in the New England Journal of Medicine that is making the rounds on news and social media platforms. The study concluded that time-restricted eating, also commonly referred to as ‘intermittent fasting’, offers no benefits in terms of weight loss, BMI, waist circumference, or other measures of metabolic health.
In this small study, two groups of obese patients were put on calorie-restriction diets. Both groups ate the same (reduced) number of calories each day and both groups lost the same amount of weight–about 17 lbs. The weight loss was achieved within the first 3-4 months of the one year study period, followed by a plateau in weight loss and then some gradual weight gain beginning at about 9 months into the calorie-restriction period.

But the group that could only eat between the hours of 8 AM and 4 PM (time-restricted eating/intermittent fasting group) did not show any further improvements compared to the group who could eat whenever they wanted to. This has led some–including some health experts–to broadcast (falsely) that fasting offers no health benefits or that ‘intermittent fasting’/time-restricted eating is still a healthy practice, even if it doesn’t translate into measurable benefits, because it might support the ability to maintain long-term calorie restriction.
To understand why these interpretations are faulty, we should start by making a critical distinction between true fasting (inducing the fasting state) and so-called intermittent fasting (IF) or time restricted eating (TRE). In short, the true fasting state does not begin, by most accounts, until 24 hours without taking in calories, while IF/TRE typically involves only 16 hours without calories. So IF/TRE stops about eight hours short of achieving the actual fasting state.
In a previous Briefing, I discussed at some length the myriad benefits of the fasting state. Taking in just water and other calorie-free liquids like coffee or tea for at least 24 hours activates the production of life-extending hormones called sirtuins; induces a state of autophagy in which the body undergoes cellular self-repair; and promotes fat burning. Critically, fasting causes all these healthy things to happen without slowing down metabolism.
By contrast, TRE/IF (hereafter TRE) does not activate sirtuin production, induce autophagy or necessarily even promote fat burning. It can be used as a weight loss tool but only if it includes calorie restriction. Eating the same number of calories in 8 hours as we normally would in 16 hours does not lead to weight loss.
And, as previously discussed, calorie restriction diets, regardless of whether they include TRE or not, only work for a few months. Prolonged calorie restriction causes metabolism to slow down. And, as metabolism slows, the daily caloric deficit (the thing that induces us to burn fat) shrinks as our body tissues learn to make do with less food. Eventually, our bodies learn to function well without having to burn any extra fat, and weight loss stops. This happens typically at about 3-4 months after beginning a calorie-restriction diet, regardless of whether or not TRE is employed.
Worst of all, once we hit the weight loss plateau caused by inducing sluggish metabolism through chronic calorie reduction, it becomes very difficult to raise our metabolism again–especially when we are older. Increasing our calories does not raise our metabolism. Even extremely prolonged exercise, which can increase our caloric demand, does not generally raise our metabolism.
Once we plateau, continuing a calorie-restricted diet no long induces weight loss causing most people to quit. But reverting to normal levels of calorie consumption–in the context of a now sluggish metabolism–causes the weight to fly back on. This is the mechanism behind the familiar yo-yo effect of dieting and the reason subsequent diets are less effective in inducing weight loss. If you look closely at the above graph, you can see that beginning to happen in the last 3 or so months of the year-long study.
In short, fasting (at least 24 hours without any calories) is one of the healthiest, most important hormetic practices available to us but TRE, which generally refers to going 12-16 hours without calories, is not hormetic because it does not induce the true fasting state that unleashes all of the astonishing health benefits. And, if practicing TRE also includes restricted caloric intake, it down-regulates metabolism which can be harmful to our long-term health.
Depression, Antidepressant Medicines, and the Brain
I. A breakthrough in our understanding of brain function has the potential to revolutionize psychiatric therapeutics
Brain cells communicate with one another through proteins called neurotransmitters, and the most abundant neurotransmitter in the brain is glutamate. Glutamate binds to receptors on brain cells, which open channels into the cell, allowing charged particles called ions to enter, causing the nerve to fire (conduct an electrical impulse along its length).
A glutamate receptor has four subunits, each of which can bind one molecule of glutamate. And nerves also have four levels of conductivity, from weakest (1) to strongest (4). Previously, it had been understood that the strength of conductivity (1 - 4) was related to the number of glutamate subunits that had been bound (two bound subunits caused a higher level of discharge than one; three caused a higher level than two, etc.).
But an important new study using cryo-electron microscopy, with sophisticated data analysis, has turned this understanding on its head. In fact, each individual subunit functions a little differently from the others and it is the pattern of subunit binding, not just the number of subunits that are bound at any given time, which determines the level of conductivity of nerve firing.
It turns out that in order for a nerve to fire, two of the subunits (A and C) must first bind to glutamate before either of the other two (B and D) can. And having all four subunits bound does not guarantee maximal (level 4) conductance. In fact, this fully bound state is more likely to cause lower levels of conductance (1 - 2). It is the sequence of subunit binding, not the degree of binding, that determines the message that is conveyed, as reflected by which of the four degrees of conductance is initiated.
Understanding this provides a potential mechanism for upregulation (or downregulation) of brain nerve cell activity–something that is central to the treatment of conditions like depression, dementia, Parkinson’s disease, and epilepsy. These findings may aid in the development of a new generation of more effective neurological and psychiatric therapies with fewer side effects (more about this below).
II. The current antidepressant medicines
The deficiency theory
We know that people who suffer from depression often have lower than normal levels of critical brain hormones called monoamine neurotransmitters (MANTs). Low concentrations of serotonin, norepinephrine, and/or dopamine have all been associated with major depressive disorder (MDD) and we have all been taught to understand this association as a cause-and-effect phenomenon (low levels of MANTs cause depression).
Why? The charitable explanation is that, based on early clinical trials showing that medicines that raise MANT levels improve symptoms of depression, it makes sense that MANT deficiencies are what cause the problem.
Antidepressant classes
Selective Serotonin Reuptake Inhibitors (SSRIs), Serotonin-Norepinephrine Reuptake Inhibitors (SNRIs), Monoamine Oxidase inhibitors (MAOIs), and tricyclic antidepressants each represent a separate class of antidepressant medicine. According to the deficiency theory, each of these medicines works by boosting particular levels of one or more MANTs. Once normal levels of these brain hormones are achieved, depression is alleviated.
However, over time, we have learned that the clinical trials that led to the approval of these medicines were not as impressive as one might think in terms of showing a clinical benefit compared to placebo. As early as 2002, a group of researchers, under the Freedom of Information act, was given access to all of the FDA clinical trial data submitted by pharmaceutical companies (Pharmas) for approval of antidepressant medicines that target MANTs.
What is particularly special about that trove of data is that, because the FDA requires Pharmas to submit all their data from all of the clinical trials they conduct, it contained many studies that didn’t show favorable outcomes and were therefore, never publicly reported.
Analysis of the full data revealed that most of the studies found MANT-raising medicines to offer no benefit or less benefit compared to placebo. Only 43% of the total randomized clinical trials (RCTs) performed demonstrated any benefit beyond that seen with placebo and even then, the differences were small. 82% of the benefits seen in the treatment cohorts (the groups that got the drug) of these minority positive-outcome studies were also seen in the placebo cohorts!
These findings were so stunning that several other groups including the FDA themselves, performed their own meta-analyses from the same (and/or similar) data sets. And they came to the same conclusion: overall, SSRIs, SNRIs, and MAOIs offer minimal benefit compared to placebo.
So, while these new-generation antidepressants correct deficiencies of serotonin, dopamine, and norepinephrine, it does not look like those deficiencies are what drive depression. In fact, studies show that lowering MANT levels in people without MDD does not cause them to develop depressive symptoms. And lowering MANT levels in patients with MDD does not make their depression worse.
All of this fits with the clinical experience of healthcare providers. Ask any psychiatrist or primary care provider and they will tell you that a substantial share of their patients do not respond to antidepressant medicines and, among those who do, the effect is oftentimes not long-lasting. For years, most medical providers have used a trial-and-error approach to prescribing antidepressant medicines, looking to achieve the right balance of MANTs. We also assumed that when, over time, these medicines become less effective, it is because patients get used to them (a physiological principle called accommodation). But these well-observed limitations are also consistent with, and are in fact better explained by, the placebo effect.
Last week, in another landmark study that is sure to make headlines, we learned that the long-term use of SSRIs and SNRIs does not make people feel better, more energetic, happier–even when they do report less depression. The purpose of treating depression is to improve patients’ quality of life but it looks like medicines that target MANTs don’t provide any measurable improvement in that regard, in the long-term.
In this extremely high-powered study, health-related quality of life (HRQoL) was measured using the SF-12 . The SF-12 is a self-reported outcome measure that assesses the impact of health on an individual's everyday life, used commonly in medicine as a quality of life measure. Patients with MDD using antidepressant medications were compared to those not on antidepressant medicines and no significant difference was found between these cohorts, leading the authors to conclude: “The real-world effect of using antidepressant medications does not continue to improve patients’ HRQoL over time.”
III. Glutamate as a target for depression
Glutamate is the brain’s most prevalent neurotransmitter and is involved in more than half of all brain nerve cell activity. Recently, it has been suggested that monoamine neurons that fire in response to MANTs, also use glutamate as a co-neurotransmitter.
Glutamate is produced from glutamine, an amino acid that is synthesized by astrocytes–specialized cells in the nervous system that provide physical and metabolic support to nerve cells. In the presence of certain enzymes (pyruvate carboxylase and glutamine synthetase) glutamine is transformed into glutamic acid or glutamate. Glutamate, as described above, binds to nerve cell receptors in specific patterns, opening ion channels and causing them to fire. Once glutamate is used, it reverts back to glutamine, which in turn gets recycled to make more glutamate.
Research shows that patients with MDD have abnormal levels of glutamate/glutamine cycling in certain key areas of the brain. For example, patients with MDD show decreased levels of glutamate/glutamine exchange in the hippocampus, an area of the brain involved in processing and storing memories, and in the cingulate cortex, part of the brain’s limbic system, which helps mediate emotions and mood.
New antidepressants are currently being developed that aim to affect the glutamate/glutamine cycle. Specifically, drugs such as ketamine which target the N-methyl-D-aspartate (NMDA) receptor (a glutamate receptor/ion channel found on neurons) is already showing some promise as reported in the April 25, 2022 Briefing, producing rapid and sustained antidepressant effects in patients with MDD.
And other compounds that target different glutamatergic mechanisms, such as GLYX-13 (a glycine-site partial agonist at NMDA receptors) appear promising in early clinical trials. Thus, the clinical findings to date are encouraging and the development of novel compounds that target these receptors and their various glutamatergic mechanisms may represent the new (and hopefully, improved) wave of antidepressant medicines.
IV. A few words about the placebo effect
Placebo, in the common vernacular, is often used to mean fake, inauthentic, imaginary–a way of casting a particular result as false. In fact, much of medicine operates to some degree by inducing a placebo effect which is defined as a beneficial outcome produced by a treatment that cannot be attributed to the properties of the treatment itself, and must therefore be due to the patient's belief in that treatment.
Whether the intervention is a pill, a shot, an acupuncture needle, or a chiropractic manipulation treatment, its success is often tied to a patient’s expectations and the setting or context in which it is delivered, as shown in the graphic below (taken from Wagner and Atlas in their excellent review of the neurological mechanisms of the placebo effect).

The relationship between negative and positive cognitions and our emotional state has been well-documented. With regard to depression, for example, it has been noted that many people with MDD are at least in part depressed about having depression–a condition marked by feelings of hopelessness. In this context, receiving a therapy from a trusted healthcare provider in a white coat who seems knowledgeable and caring can induce some measure of hope. Lifting the veil of hopelessness can alleviate some of the depression of MDD.
So, is it unreasonable to prescribe a medicine such as an SSRI or SNRI, designed to raise MANT levels, even if we understand its benefit to come mainly from the placebo effect?
Here’s my take: Until better (possibly glutamatergic) medicines are available to safely and effectively treat MDD, that calculation will have to be made at least in part by healthcare providers on a case-by-case basis. There is no doubt that these medicines–whether from placebo or as a result of the small extra benefits that some sufferers of MDD derive from their use–have saved some patients’ lives. Primary care providers, psychotherapists, and psychiatrists should endeavor to build the strongest possible bonds of trust with each other and with their mutual patients suffering from major depression. Only through networks held together by such bonds of mutual trust and respect will it be possible to have confidence in obtaining the granular feedback and degree of surveillance needed to shepherd patients with MDD through their darkest times, using these medicines.
We know that psychotherapy combined with MANT-targeting medicines works better for MDD than either therapy or medication alone, so this should be de rigueur. We also know that other non-pharmaceutical interventions have been shown to improve MDD. Transcranial magnetic stimulation (TMS) is a non-invasive form of treatment in which a changing magnetic field is used to cause electrical activity in specific brain areas leading to improvement in depression. Cardiovascular exercise, sauna bathing, and prolonged contact with nature have similarly shown positive effects when engaged in regularly and they have the added benefits, compared to MANT-directed medicines, of having no negative side effects and providing results that do not wane over time.
A holistic approach to the treatment of MDD may involve bringing patients’ family members and friends into the strategy to help set up and reinforce healthy routines such as swimming, hiking, or other activities that engage the cardiopulmonary system and put patients in contact with trees, grass, lakes, sunlight, mountain, ocean, etc. It may also involve bringing in allied healthcare professionals to help reinforce the message and encourage patients to push back against the inertia of hopelessness. Current antidepressants that target MANTs may be part of the treatment but probably should not be used as a mono-therapy nor viewed as a long-term fix. Community, connection, and caring are often the missing ingredients in the treatment of patients with depression.
Fetal brain development is dysregulated by in-utero maternal depression and anxiety
In a new study, fetal brain volume and cortical folding were measured using MRI, and fetal brain creatine and choline were quantified using proton magnetic resonance spectroscopy. Infant neurodevelopment was measured using validated scales and assessments at 18 months.
While in the womb, the researchers observed some minimal alterations in creatine and choline levels but significant changes in the developing brain anatomy of the fetuses of women experiencing chronic stress, anxiety, and/or depression. The main changes were altered sulcal depth and diminished volume of the left hippocampus (an area of the brain that deals with processing and laying down memory), which the authors believe impacted the neurodevelopment issues seen at 18 months.
These children are expected to be at increased risk for developing persistent social-emotional problems including difficulty establishing positive relationships with others, including their mothers.
This is a small but interesting study. It represents a ‘signal’ from the data, rather than a definitive conclusion about maternal depression/anxiety and fetal development. But it points to the need for medical, environmental, and social-emotional support for pregnant women and possibly also for early intervention in infants and toddlers born following particularly stressful pregnancies. I can only imagine what it might mean to expecting parents in Ukraine at this moment.
https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2791732
COVID-Corner
The daily case rate of COVID-19 (C19) in the US is no longer knowable. Only lab-performed PCR-positive tests reported to public health departments inform that statistic. In many cases, infected people are no longer getting tested. And if they do, they are more likely to use a home test which is more available and less expensive than a PCR test and gives fast results. But home tests don’t get included in the official statistics. Public health experts now estimate that the official reported case rate reflects between 1/5 and 1/10 of the actual rate and that’s a wide variance.
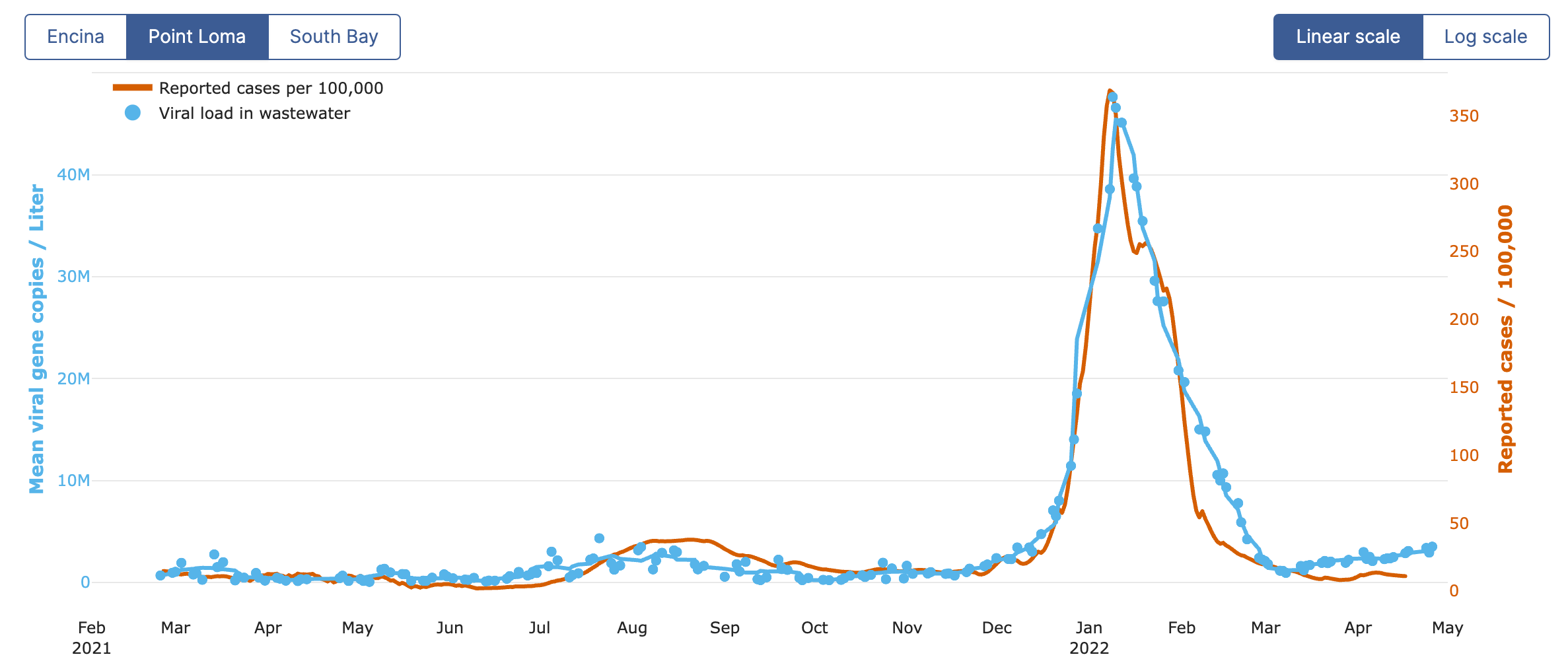
Wastewater surveillance is a better method for tracking C19 at a community level. While it cannot provide a case rate, measuring the amount of SARS-CoV-2 virus in wastewater can tell us with high accuracy whether cases are going up, down, or remaining the same.
Here in San Diego, UCSD has done a tremendous job monitoring the wastewater and sending out alerts to the community when levels of the virus go suddenly way up. However, less violent spikes do not make the news. As we see in the following graph, C19 in San Diego is again steadily on the rise and is currently at the highest level it has been during the pandemic, prior to the Omicron wave.
But this is no longer a news story. As discussed in a prior Briefing, C19 has been falsely labeled as ‘endemic’ to support a change in messaging on the part of public health departments across the US (and the world). “It’s time to stop reporting cases,” many experts began saying late last year, “and focus on hospitalizations and deaths.” And that’s essentially what has happened.
Meanwhile, the virus continues to mutate in ways that help it spread ever faster. The newest variant, BA2.12.1 is 25% more transmissible than BA.2, which was 30% more transmissible than Omicron (BA.1), which was 50% more transmissible than Delta, which was 50% more transmissible than Alpha, which was more transmissible than the original strain D614G that caused the first wave of cases in the US. And as the virus injures the brains and other organs of even those who get mild cases, and induces chronic illness in about a third of those who get infected (long-covid), the long-term consequences of C19 are as yet unknown.
Now, two new sub-lineages of Omicron have been discovered in South Africa. BA.4 and BA.5 are yet more transmissible and it looks like they are mutated far enough from BA.1 that prior infection with Omicron offers little protection against infection with the new variants. Even prior infection plus vaccination offers only mild protection against infection.
Here at the office, our masks are staying on, and I recommend that all my patients continue to take basic precautions like masking and getting your booster shots to lower your risk of infection. This is important for everyone but especially children, most of whom are unvaccinated and who potentially have the most to lose in terms of long-term health and longevity following even mild C19 infections.