

COVID-19 Weekly Briefing for Monday, April 4, 2022
C19 is not yet endemic; sauna bathing improves healthspan and lifespan; and I'm sticking with Moderna for my second booster as BA.2 ramps up: here's why...

Disinformation in the time of COVID-19; the stunning health benefits of sauna bathing; which vaccine should you take for your second booster; and a review of long-covid (LC) and organ tissue injury (OTI) following SARS-CoV-2 infections.
The pandemic is over! (and other ‘alternative facts’)
Most of the world’s leading public health experts now seem united about one thing: after two years of discomfort and anxiety, we must now declare the pandemic over and return to living as we did before COVID-19 (C19). To this end, respected public health and infectious disease experts, as well as many governments, are now promoting three useful fictions.
The first is that SARS-CoV-2 (Scov2), the virus that causes C19, is now endemic. In this context, labeling a pathogen as endemic is shorthand for downgrading it to an acceptable risk of normal, everyday life.
I spent some time in a prior Weekly Briefing debunking this particular bit of disinformation but, in a nutshell, a pathogen or disease is actually endemic when both:
It has established itself permanently in the human population and:
It is stable, predictable, and does not pose a threat to the healthcare system or require the enactment of any special public health measures to keep it from spreading out of control.
It would be hard to argue against the fact that Scov2 is here to stay. But it would be equally hard to make the case, with new, highly mutated variants of concern (VOCs) emerging with ever increasing frequency to cause highly variable waves of infections with variable degrees virulence and ever-increasing transmissibility, that the virus or disease is currently stable or predictable.
The second useful fiction comes in two mutually exclusive variations of ‘alternative facts’ (a term coined by Kellyanne Conway, a political disinformation expert, to refer to lies told as truths in support of a political objective): the vaccines don’t work and the vaccines work so well that once a person is vaccinated, they no longer need to worry about catching or spreading C19.
The former lie (they don’t work) is currently being used as both validation for not getting boosted and a reason to give up on trying to protect oneself (or others) from getting infected. If the disease is everywhere and the vaccines don’t work, shouldn’t we just accept that we’re all going to get C19 and move on with our lives?
The latter lie (that once you’re vaccinated, you’re safe to drop all other protections) is being used to put an end to the inconveniences of masking, quarantining/isolating, and limiting the size of gatherings.
But the truth rarely lies in the extremes. As discussed at length in last week’s Briefing, up-to-date vaccination (now four shots for most adults) cannot eliminate the the risk of infection with Omicron or BA.2, the new dominant variant, but it can reduce it substantially. Similarly, it cannot eliminate the risk of long-covid (LC) following breakthrough infections (infections among vaccinated people) but it does reduce it by about half. And it does not guarantee absolute protection against hospitalization or death but it reduces those risks dramatically.
In short, vaccination protects us but not fully. Therefore, we should be up-to-date with our vaccinations and also continue to avoid crowds and mask around people outside of our households. For a little while longer, anyway.
The third useful fiction is that infections don’t matter; only hospitalizations and deaths do. Left out of this calculation is a veritable mountain of data showing that C19 is causing an unprecedented rate of chronic illness among those who get so-called ‘mild’ infections–the kind that don’t result in hospitalization. The long-term effects of these post-covid conditions are likely to impact the long-term health and work productivity of tens of millions of Americans for years–perhaps decades–to come.
But before we discuss long-covid (LC) and organ tissue injury (OTI), I wanted to first return to the concept of hormesis–the idea that certain kinds of stressors are good for our health–as it relates to a practice that is common in many parts of the world: sauna bathing.
I. Daily sauna bathing increases healthspan
At our practice, we promote a strategy that supports the concept of healthspan–essentially, the amount of time one spends living in good health. Healthspan speaks to quality of life, which many of us hold to be even more important than longevity itself.
Our bodies change as we age and acceptance of some decline in stamina, strength, speed, and mental acuity is probably essential for our happiness. But what we do, including how we choose to eat, work, and live, can speed up, slow down, and in some cases, even reverse aspects of physical and mental decline. In other words, humans have the possibility of increasing their healthspan.
Regular fasting, creating a sustainable and intelligent exercise routine, taking the right supplements (more about this in a future Weekly Briefing) including nicotinamide riboside (NR), resveratrol, and n-acetyl cysteine (NAC), and eating a modified Mediterranean-style diet rich in naturally occurring fiber and healthy fats that helps maintain stable blood sugar, decrease visceral fat (the fat in and around our internal organs), and promote a robustly diversified gut microbiome, each plays a role in extending both lifespan and healthspan.
So does stimulating the production of life-extending enzymatic proteins called sirtuins and heat shock proteins which are released when we engage in hormetic practices such as raising (or lowering) our core body temperature for sustained periods of time. Prolonged exercise, fasting, cold plunges, hot baths, and saunas all activate genetic pathways that improve health and extend life, making these particular stressors hormetic when engaged in routinely.
Sirtuin production is part of hormesis
Sirtuins are a family of proteins involved in regulating metabolism and aging found in nearly all life forms from yeast to humans. They are relatively consistent from organism to organism (although humans have more than yeast do) and, working in conjunction with a coenzyme called NAD, influence such things as programmed cell death (apoptosis), inflammation, and stress resistance.
There are 7 sirtuins (SIRT1 - SRT7) in humans, each playing a role in lifespan and healthspan. For example, SIRT1 is thought to be responsible, in large part, for the cardiometabolic benefits of fasting and exercise and appears to delay key aspects of aging, including protecting against a decline in vascular endothelial function (the health of the linings of our blood vessels). Increasing levels of SIRT2, slows down aging and increases longevity in mammals and in yeast. And SIRT3 appears to protect against development of abnormal blood lipids.
With increasing age, however, both NAD and sirtuin levels steadily decline, and this is exacerbated by obesity and sedentary lifestyle. Sirtuins are released during the fasting state to improve energy efficiency and alertness. And they are stimulated during prolonged exposure to heat, cold, or exercise. Increasing NAD and sirtuin levels induces health benefits in a wide range of age-related cardiovascular and metabolic disease models.
Declining NAD levels can be restored by supplementing with NAD precursors (we recommend using Tru Niagen–something that I take as a daily supplement). Increasing NAD levels has been shown to dramatically improve various age-associated functional deficits including the slowing or even reversing of diabetes, cardiovascular disease (CVD), and neurodegenerative diseases.
Since sirtuins can be upregulated by regular exercise, fasting, and prolonged exposure to extremes of temperature. It makes sense that a combination of NAD precursor supplementation and sirtuin upregulation/activation through hormetic practices may be an effective anti-aging strategy.
Science and sauna
A big advance in the field of anti-aging came in 2015 with a landmark study from Finland published in JAMA, showing that men who used sauna 2–3 times per week had a 27% reduction in risk of CVD mortality compared to those who only used the sauna once weekly, while men who sauna bathed 4–7 times per week had a 50% lower risk of CVD mortality.
Even more impressive was that the risk of all-cause mortality (death for any reason) was reduced by 40% among frequent sauna bathers compared to infrequent ones. Can you imagine a medicine that has no side effects, improves mood, energy, and sleep quality, and reduces the risk of dying from any cause by 40%? Such a drug would surely be touted as a miracle of modern medicine–the fountain of youth.
The use of sauna to extend healthspan and lifespan has subsequently become the subject of a considerable body of research. From the Finnish study, we learned that men who sauna-bathed 4–7 times per week had a 66% lower risk of developing dementia including Alzheimer's disease compared to those who sauna-bathed only once per week.
In Japan, Waon therapy, which involves 15 to 30-minutes of infrared sauna heated to approximately 140 degrees followed by a 30-minute session of lying flat on their backs covered in warm blankets, has been associated with improvements in congestive heart failure and peripheral artery disease.
And the practice of raising core body temperature has been shown to improve depression, heal chronic ulcers and other wounds, reduce chronic widespread body pain such as that seen in fibromyalgia, and even improve outcomes for cancers. And such studies form just the tip of the iceberg with regard to the known health benefits of regular sauna bathing.
Another part of hormesis involves ‘heat shock proteins’
Prolonged exposure to high heat has immediate physiological effects including increasing cardiac output (the amount of blood the heart pumps to the rest of the body) and high volume sweating which has been shown to improve the excretion of toxic heavy metals including aluminum by 3.75-fold (compared to elimination through the urine), cadmium by 25-fold, cobalt by 7-fold, and lead by 17-fold.
Repeated exposure to high heat such as regular sauna bathing induces hormetic responses similar to those seen from regular cardiovascular and strength training exercise, fasting (see the March , 2022 Weekly Briefing), and cryotherapy (prolonged exposure to extreme cold). These hormetic practices trigger a vast array of protective mechanisms that repair cell damage and activate genetic pathways that improve both lifespan and healthspan.
Part of the process of aging and the development of many chronic diseases involves the unfolding and stiffening of proteins which impairs their ability to perform their intended functions. Proteins must be supple enough to twist and fold in order to bind to things like cell receptors and initiate specific biochemical activities needed for cellular health.
In addition to sirtuins, heat stress from sauna bathing induces the production of heat shock proteins (HSPs). HSPs help repair or re-synthesize stiff, damaged proteins associated with aging–a process similar to autophagy which is induced during prolonged fasting (see the March 21, 2022 Weekly Briefing for details). HSPs have been shown to slow down neurodegenerative diseases and even the aging process itself, reduce muscle atrophy during periods of immobilization, and improve the function of mitochondria (the energy centers of our cells).
Heat stress robustly increases intracellular levels of HSPs in humans with studies showing that just 30 minutes of sauna bathing can raise HSP levels 49%. Just six days of heat therapy has been shown to increase ambient levels of HSP in men by 45% and in women by 38% and dramatically improve mitochondrial function.
And, like sirtuins, HSPs are associated with human longevity. A population-based study from Denmark showed that those who had a genetic variance leading to higher production of inflammation-lowering HSPs lived, on average, a year longer than those who did not have that genetic variance.
For those of you who have been following my work over the years, you know my belief that, in the big picture, aging and chronic diseases are mediated by progressively escalating inflammation and progressively diminishing circulation. My anti-aging strategy is to create an enjoyable lifestyle that reverses these trends of aging.
Tissue aging includes the stiffening of arterial walls (endothelial dysfunction or atherosclerosis) in the context of diminishing production of vasodilators (agents, including naturally occurring enzymes and hormones, that cause blood vessels to open, improving blood flow) and increasing secretion of vasoconstrictors (substances that narrow blood vessels to inhibit the flow of blood).
Just two weeks of sauna therapy in patients with congestive heart failure has been shown to improve endothelial and cardiac function, in part through increasing the production of natural vasodilators and reducing the production of vasoconstrictors.
Along with exercising and fasting, regular sauna bathing is one of the most healthspan and lifespan-inducing behaviors we can roll into our anti-aging lifestyle. The practice of sauna bathing not only acclimates us to temperature extremes, it induces whole-body adaptations that reduce inflammation, improve circulation, clear out old senescent proteins and cells, improve mitochondrial and protein function, and extend lifespan.
I recommend between 30 - 50 minutes of sauna bathing 5-6 times per week. If you don’t have access to a sauna room, you can use the Higher Dose infrared sauna blankets. You can order them directly from the company or, to receive a significant discount, through the office.
My wife and I sauna bathe together in our Higher Dose sauna blankets about 4-6 times per week. We listen to music or an interesting podcast, play word games, and catch up with each other amidst the seemingly relentless busyness of our lives. It has become part of our routine and that’s the way to benefit from a health practice. Whether it’s exercise, meditation, a low-glycemic load diet, or any other health practice, the secret to success lies in consistency.
II. Omicron and BA.2 are less virulent but for many, there is more to C19 than the acute period of infection.
Long-covid (LC) and organ tissue injury (OTI)
By way of review, long-covid (LC) refers to people who, after a SARS-CoV-2 infection, go on to have chronic symptoms. For some people, LC presents as a continuation of the acute infection–they get sick with C19 and then just never seem to recover. For others, LC comes on weeks or even months after the acute C19 infection has resolved. For this group, LC feels like a relapse or second infection that doesn’t resolve in a timely way.
LC can affect people who have asymptomatic, mild, or severe acute infections but seems to be more common among those who who develop five or more C19 symptoms during the acute infection. Such patients are also more likely to progress to hospitalization and ICU care. LC can affect children, teens, and adults of all ages.
The amount of people who go on to LC is not known but the lowest estimates are alarmingly high.
In this study from Norway, including mild (non-hospitalized) acute C19 infections and severe (hospitalized) ones, at 6 months, 61% of all patients had persistent symptoms. 52% of young adults with mild cases (aged 16–30) had symptoms at 6 months, including loss of taste and/or smell (28%), fatigue (21%), shortness of breath (13%), impaired concentration (13%) and memory problems (11%).
In this high-powered retrospective study of > 80 million people, 57% had one or more LC symptoms at 6 months after C19 diagnosis including difficulty breathing (19%), fatigue/malaise (13%), headache (9%), abdominal symptoms (16%), body aches (3%), cognitive symptoms (8%), and anxiety/depression (23%). Interestingly, these symptoms were significantly higher among those who had C19 compared to those who, during the same time period, had flu. The risk of LC was higher among patients who had more severe acute infections, females, and young adults.
A recent study showed that up to 50% of children who get C19 progress to LC. And, in a recent review of eighteen studies that followed patients for at least one-year after C19 diagnosis, 28% were still reporting fatigue/weakness, 18% had difficulty breathing, 26% had body aches, 23% had depression or anxiety, 19% had memory loss, and 18% still had difficulty concentrating at least one year after their acute infections.
In short, while we do not yet know how many people will go on to LC, the numbers are frighteningly high and include children and young adults who experienced only mild or even asymptomatic acute infections. These people, with the majority of their lives ahead of them, have the most to lose from developing chronic illness at an early age and yet, they are being encouraged by public health authorities the world over, including here in the US, to stop masking and return to high-density congregate activities like restaurant dining, concerts, schools, and sporting matches.
And LC is just one of the concerns for those who contract C19. In prior Weekly Briefings, I discussed the astonishingly high number of people who go on to have multiple signs of autoimmunity following infections with Scov2. The UK Biobank study demonstrated how those who had C19 lost part of their brain (gray matter in the area that mediates smell and memory) compared to those who did not get C19 by comparing MRI scans on both groups before and during the pandemic. We have seen reductions in sperm count, loss of kidney function, scarring in the lungs and on the heart, an increased rate of stroke, multiple sclerosis, depression, anxiety, and, as discussed in last week’s Briefing, a 40% increase in the risk of developing diabetes within a year among those who got C19 compared to those who did not.
Vaccination helps
Preliminary data suggest that primary vaccination (2 shots) lowers the risk of developing LC. One fairly high-powered study from the UK which used the ZOE COVID symptom study app showed that vaccinated persons are far less likely (about 49% reduction in risk) to progress to LC.
And this study from Israel of around 1,500 vaccinated health-care workers, found that 19% of the breakthrough infections produced symptoms that lingered for more than 6 weeks. That would represent a significantly lower rate of LC compared to studies which included many unvaccinated people (although smaller studies like this one are less reliable). In this recent study, vaccination reduced the risk of LC by about 41% in more than 3,000 double-vaccinated participants who experienced breakthrough C19 infections.
It is worth noting that, while most studies point to a reduction in progression to LC among vaccinated compared to unvaccinated people who get infected, there is at least one high-powered study to the contrary, showing that while vaccination was highly protective against hospitalizations, deaths, ICU admittance, and other severe outcomes associated with acute infection, it did not seem to significantly reduce the risk of LC.
That said, vaccination certainly reduces the risk of infection, and the best way to not get LC is to not get infected. Avoiding crowds and wearing an N-95-equivalent mask help and this, in my view, is something that the premier public health agencies and experts should be advising us all to do. Politicians may have a different (and perhaps valid) agenda but public health and infectious disease experts should, I believe, stick to what they know. As the disastrous communication efforts of the CDC demonstrate well, scientists are not great at politics.
III. Which booster should you take?
Antibodies, T cells, and correlates of protection (COPs)
Antibodies are proteins (made by specialized immune cells called B cells) that stick to pathogens and gum them up. They also bind to other cells of the immune system to stimulate them and help coordinate self-defense.
Antibodies contain what’s called a fragment crystallizable region (Fc region) at their tip (the ‘tail end’) which interacts with receptors on immune cells and with other proteins that activate the complement system–part of the innate immune system that enhances (complements) the ability of antibodies and immune cells to do their jobs.
Antibodies play a big role in immunity and neutralizing antibodies (NAs) in particular, which gum up a pathogen well enough to render it incapable of making copies of itself, have been used as what is known as a ‘correlate of protection’ (COP) against infectious disease. A high enough titer (amount) of NAs indicates that you are protected against disease.
NAs are not the only potential COP against C19. T cells (immune cells that kill infected cells and also help coordinate immunity) are another, and many infectious disease experts have looked more to T-cells than to NAs when assessing protection against severe disease (hospitalization) or death.
The Moderna and Pfizer vaccines: same-same but different
The Moderna and Pfizer mRNA vaccines work the same way: they introduce code (mRNA) into our bodies’ cells that orders them to make a protein found on the Scov2 virus, called the spike. Spike proteins are the stippled bits that stick out from the coronavirus’s surface like a crown (hence ‘coronavirus’).
Spikes cannot cause infections by themselves but they are ‘foreign’ proteins not normally found in our bodies, so when our cells make some spike proteins, this activates the immune system to build antibodies and T cells to attack them.
And although the Moderna and Pfizer vaccines induce comparable neutralizing antibody titers and T cell responses, data throughout the pandemic have shown Moderna to elicit stronger and longer protection against symptomatic infection compared to Pfizer in the real world. Why should this be?
In the past, I have pointed to two factors that could likely make Moderna a little more protective. The first is that primary vaccination with Moderna used a longer inter-dose interval compared to Pfizer (four weeks between shots v. three weeks) and we now know that a longer inter-dose interval helps these vaccines to work better. In fact, it is now estimated that a 16-week inter-dose interval is probably ideal for inducing the strongest level of protection.
However, the inter-dose interval seems less likely to be informing the better performance of Moderna compared to Pfizer when used many months later, as a booster.
The second factor that might give Moderna the edge (and the one that has made the most sense to me) is that Moderna uses a bigger dose of mRNA (100 mcg compared to Pfizer’s 30 mcg). Even as a booster, Moderna’s half-shot (50 mcg) is still nearly double that of Pfizer’s full shot (30 mcg).
It seems intuitive that a bigger dose of code would mean a stronger and more lasting immune response. It also correlates to the overall slightly higher degree of immunity symptoms (the flu-like side effects) that some people experience following vaccination with Moderna compared to Pfizer.
This understanding informed last week’s Briefing, wherein I noted that I would be taking a fourth shot of Moderna as my (second) booster shot. In my mind, I’ll take 12 hours of feeling like I have the flu to lower my risk of developing LC, OTI, or diseases like dementia and diabetes.
But this past week, a new study published in Science offers new observations about the relative immunity induced by the two current mRNA vaccines, leading some experts to suggest that it might be beneficial to mix them rather than sticking with the same vaccine for every dose.
Let’s go back to the concept of COP, which is what getting immunized is all about. We know that neutralizing antibody titers and T cell titers have been proposed as COPs against C19. But what about that antibody-mediated effector function induced by the Fc region of antibodies? Fc function has also been shown to play a critical role in vaccine-mediated protection against Scov2 infection.
The new study compared the Fc-functional performance of the Moderna and Pfizer vaccines against spike proteins from various prior VOCs including the ancestral wild-type strain, Alpha, Beta, Gamma, Kappa, and Delta, and found that Moderna outperformed Pfizer.
What’s more, Moderna seems to produce higher titers of IgA–the class of antibodies that act at the mucous membranes that line our airways and intestines. We know that Scov2 enters our bodies through these membranes and antibodies that attack the virus there, before it can get inside us, might be the key to developing protection against infection.
In previous Weekly Briefings, I have written extensively about the need for new vaccines that are sprayed into the nose or swallowed as pills (rather than shot into a muscle in the arm). Intranasal or oral vaccines would induce more IgA and therefore, likely give us better protection against infections. Prior studies have demonstrated that IgA has strong antiviral properties against Scov2 and is likely critical for vaccine efficacy (VE) against infections.
However, the new study also went on to reveal that while Moderna outperformed Pfizer with regard to Fc effector function and IgA production, the Pfizer vaccine produced stronger IgM and IgG responses compared to Moderna.
IgM is the first subclass of antibodies produced in response to a pathogen once it has crossed the mucous membranes and penetrated into the body’s interior to cause an infection. In the case of C19, IgM comes on about a week after infection and then shuts off about two weeks later. It is mainly responsible for fighting the virus during the acute phase of infection.
IgG antibodies come on about two weeks after infection to help finish off whatever virus is still remaining and then hang around for months or years, acting as sentinels on the lookout for the reappearance of Scov2.
Standard antibody tests look for both IgM and IgG. If only IgM is present, that means you are at the beginning of the infection (within the first 2 weeks). If both are present, that means you got infected about 2 - 3 weeks ago. If only IgG is present, that means you had an infection at least 3 weeks ago but possibly many months ago or longer.
So, for some reason, perhaps because of the different doses or maybe because the fatty envelopes that the mRNA code comes wrapped in are different between the vaccines, Moderna and Pfizer provoke slightly different immune responses. Moderna stimulates better Fc effector function and more IgA while Pfizer stimulates more IgM and IgG.
We don’t yet know which of these differences (if any) are mainly responsible for the slightly better protection Moderna seems to afford compared to Pfizer. And some leading experts, including Eric Topol (see March 29, 2022), are at least suggesting that a mix-and-match approach could be a smart strategy when considering which vaccine to take as your second booster shot. So, if you got Moderna for your last shot, should you now get Pfizer for your next one (and vice versa)?
Here’s my take: I do not presume to understand this science better than Dr. Topol and if he makes a declarative recommendation that we mix vaccines, I will follow his guidance. However, insomuch as he is only raising this idea as a possible strategy, I’m going to stick with my original plan to get a fourth shot of Moderna vaccine which produces more IgA–the antibody subclass that patrols the airways and gut, as I think this will offer better protection against infection.
Since even mild infections can lead to LC, OTI, and chronic diseases (long-term health consequences), my focus, contrary to the now dominant narrative that focuses exclusively on preventing hospitalizations and deaths, is to do everything I reasonably can to avoid getting infected while expanding my activities judiciously.
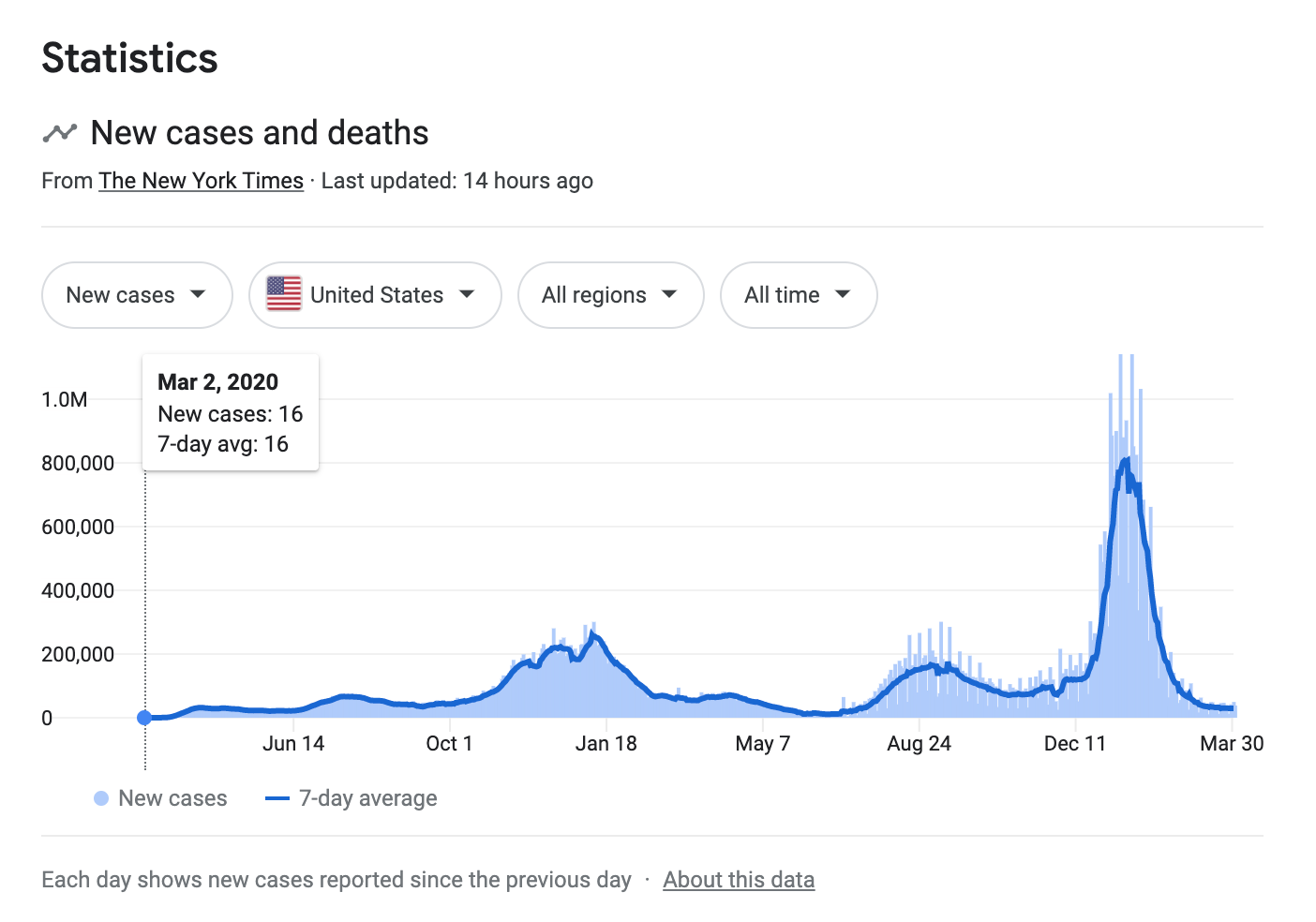
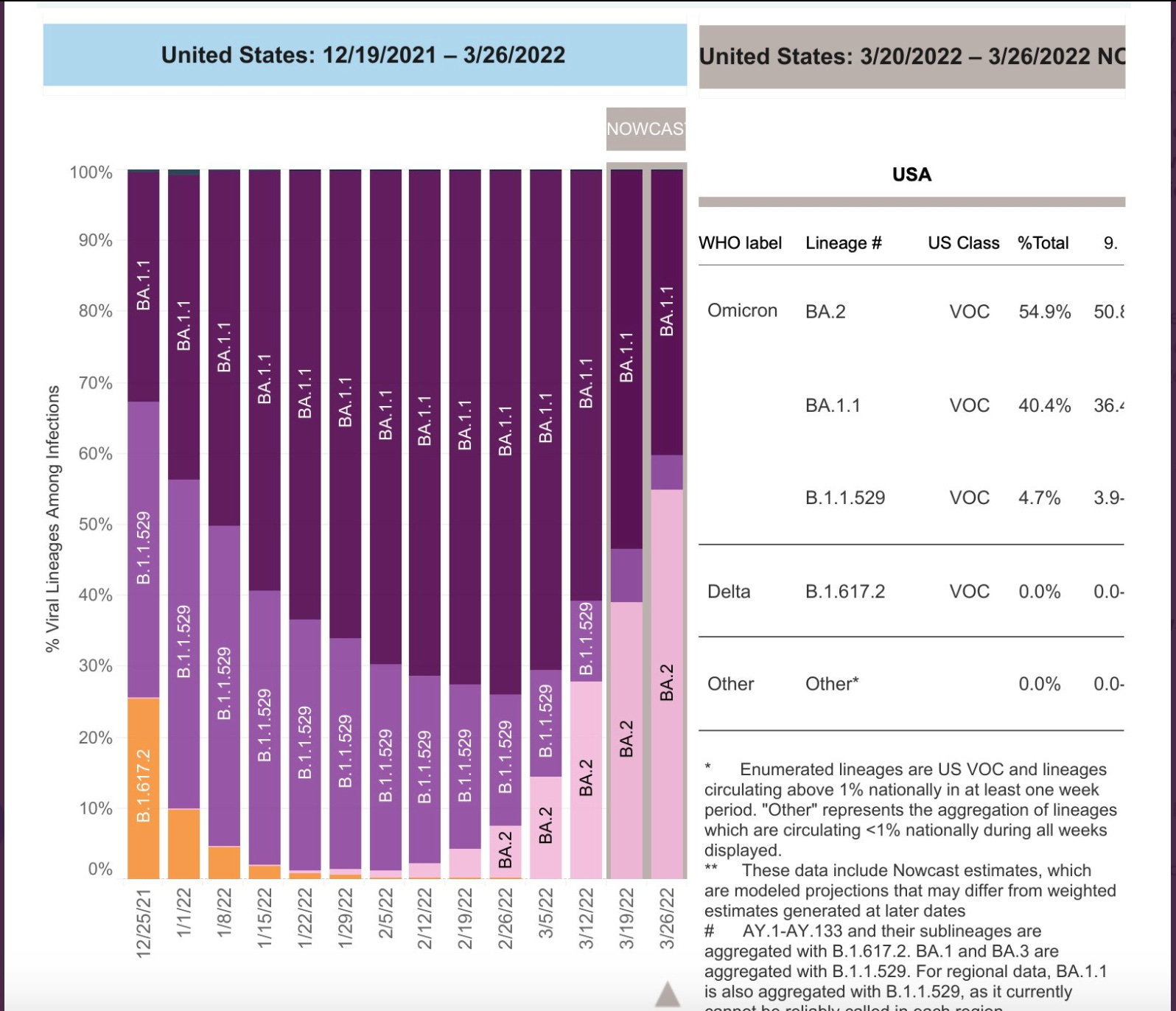
IV. BA.2 update
As predicted, BA.2 is now the dominant variant in the US.
So, what do we know so far about BA.2? Compared to Omicron, a few months ago considered to be possibly the most contagious virus known to mankind, BA.2 is 30% more transmissible, has double the viral load, and is associated with a 70% reduction in neutralizing antibodies among those with prior immunity.
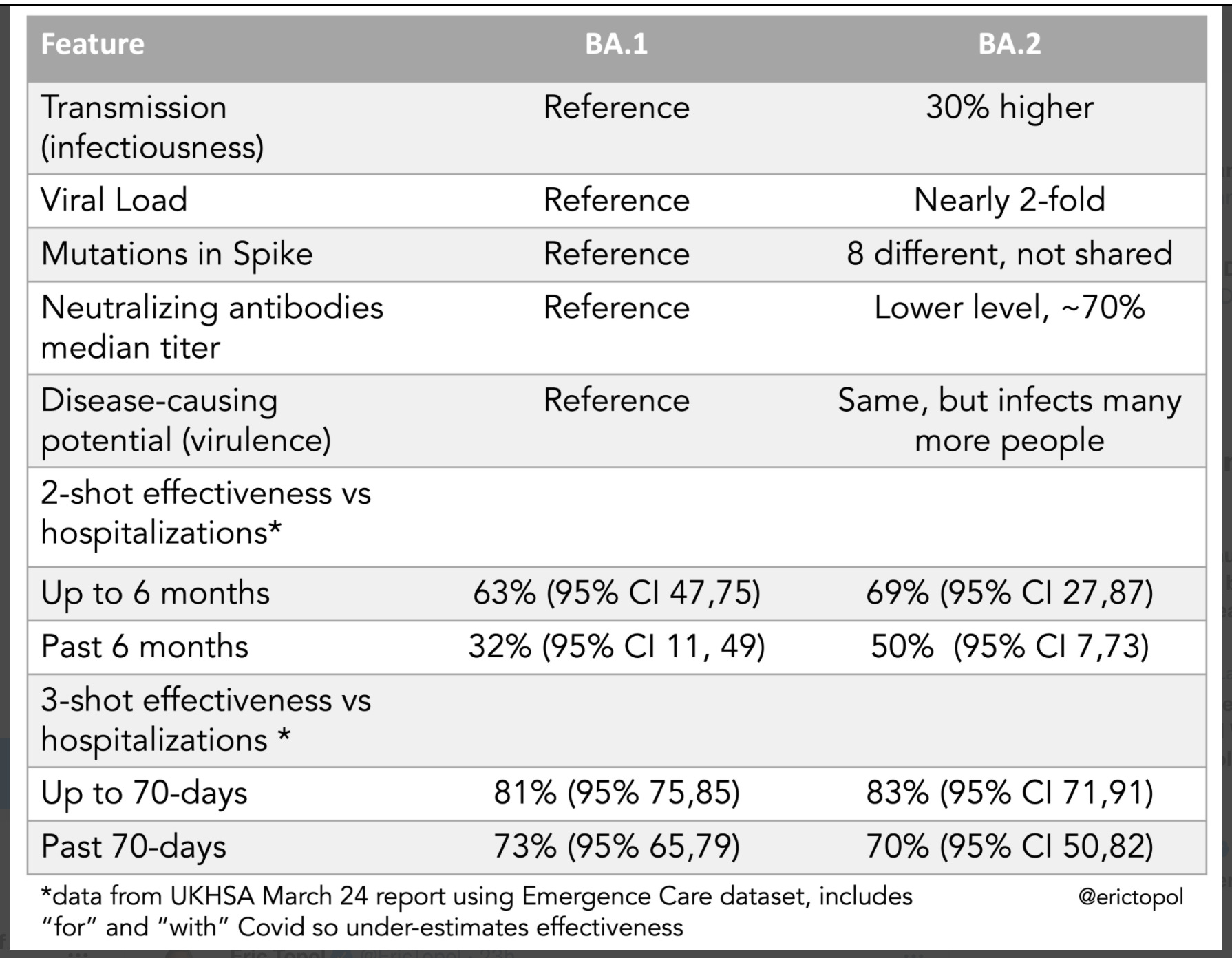
On the plus side, while there were some early indications that BA.2 might be more virulent, and new data are showing that it is more virulent among children, the public health experts at CDC and UKHSA do not think it is significantly more virulent overall. And, strangely, despite lower neutralizing antibody titers, the vaccines are working just as well or a little better against BA.2 than they did against Omicron in terms of protection against severe disease.
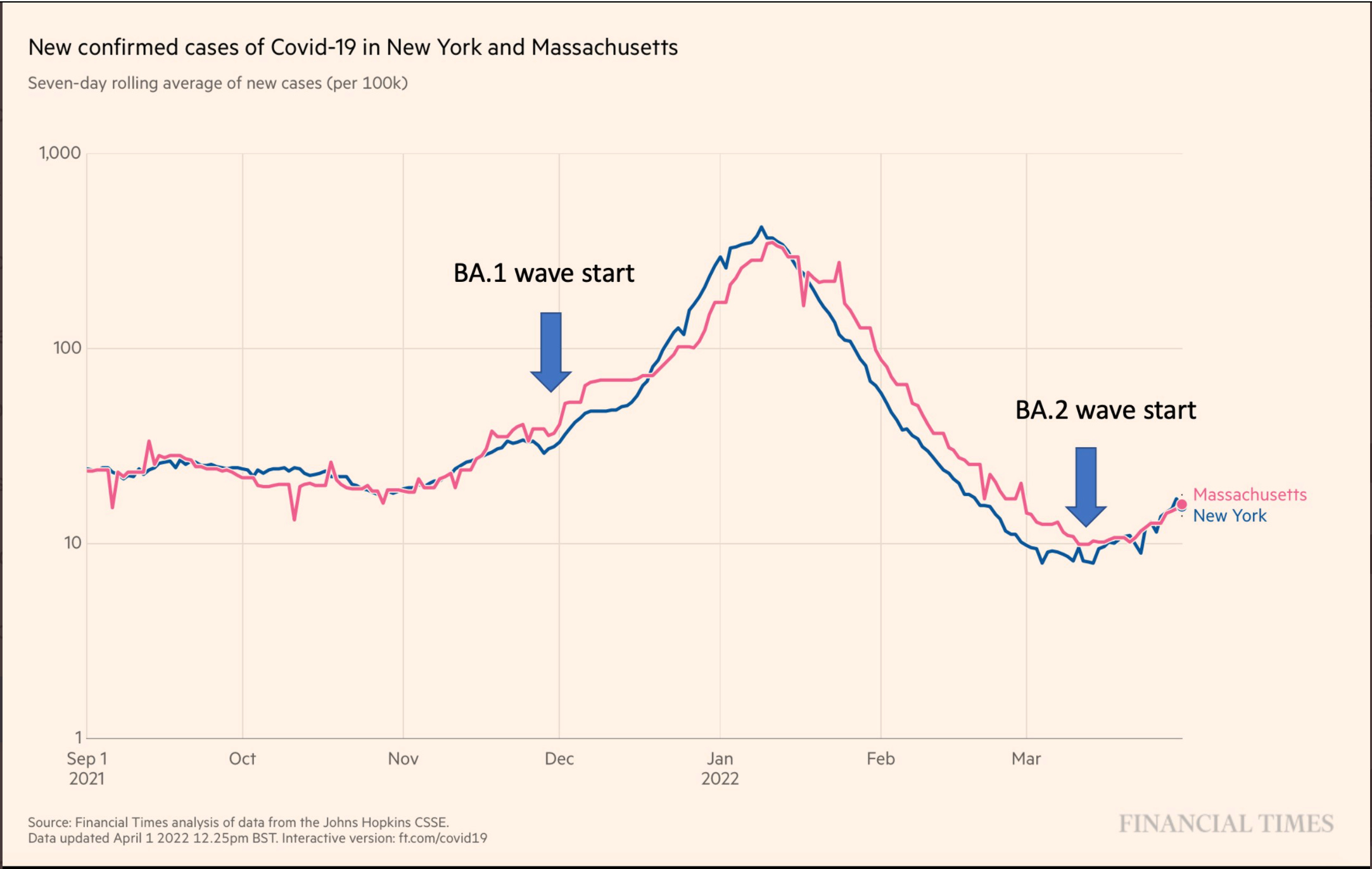
So where are we with regard to the BA.2 wave? As predicted, it has started in the Northeast.
How big of a wave we will see is anybody’s guess but we should keep in mind that the CDC only tracks positive PCR tests to publish this data and, as we know, with very few people seeking PCR tests (rapid/at-home tests are less expensive, more convenient, and now more popular; also, fewer people are getting testing of any kind since Omicron is in most cases less severe and can easily pass for a cold), whatever numbers they publish will undoubtedly represent a significant undercount.
Meanwhile, wastewater surveillance, which represents a more accurate picture of the community prevalence of Scov2, continues to show increasing dominance of BA.2 and increasing levels of the virus here in San Diego. We are likely not far behind states like NY and MA. We’ll be keeping our masks in place at the office for a while still…